Osakunor Derick Nii Mensah, Mduluza Takafira, Midzi Nicholas, Chase-Topping Margo, Mutsaka-Makuvaza Masceline Jenipher, Chimponda Theresa, Eyoh Enwono, Mduluza Tariro, Pfavayi Lorraine Tsitsi, Wami Welcome Mkululi, Amanfo Seth Appiah, Murray Janice, Tshuma Clement, Woolhouse Mark Edward John, Mutapi Francisca
Centre for Infection, Immunity and Evolution, Institute of Immunology and Infection Research, University of Edinburgh, Edinburgh, UK.
Department of Biochemistry, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe.
BMJ Glob Health. 2018 Mar 27;3(2):e000661. doi: 10.1136/bmjgh-2017-000661. eCollection 2018.
Recent research has shown that in schistosome-endemic areas preschool-aged children (PSAC), that is, ≤5 years, are at risk of infection. However, there exists a knowledge gap on the dynamics of infection and morbidity in this age group. In this study, we determined the incidence and dynamics of the first urogenital schistosome infections, morbidity and treatment in PSAC.
Children (6 months to 5 years) were recruited and followed up for 12 months. Baseline demographics, anthropometric and parasitology data were collected from 1502 children. Urinary morbidity was assessed by haematuria and growth-related morbidity was assessed using standard WHO anthropometric indices. Children negative for infection were followed up quarterly to determine infection and morbidity incidence.
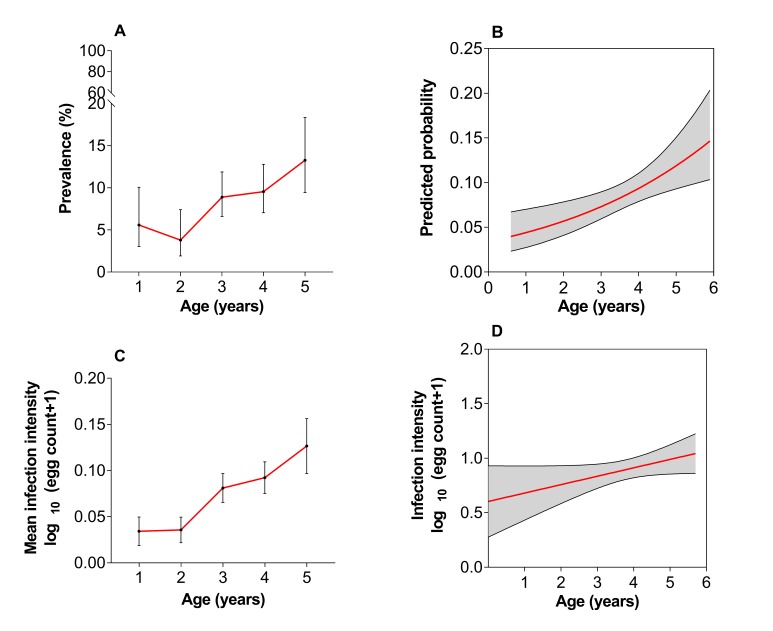
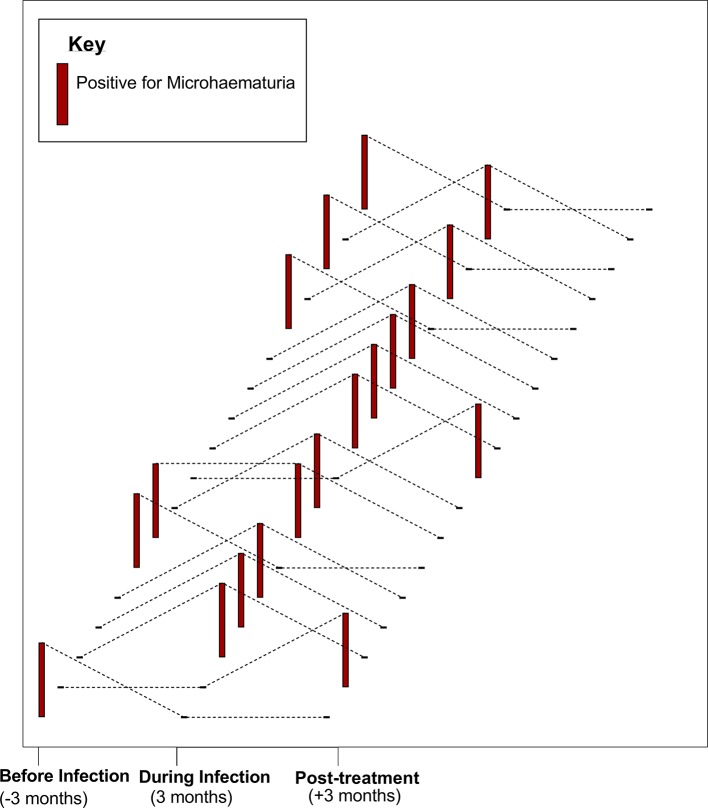
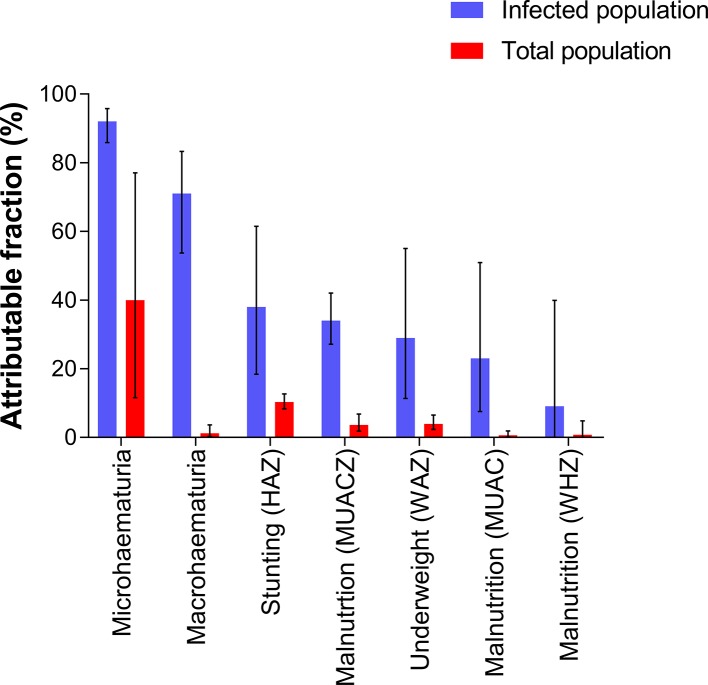
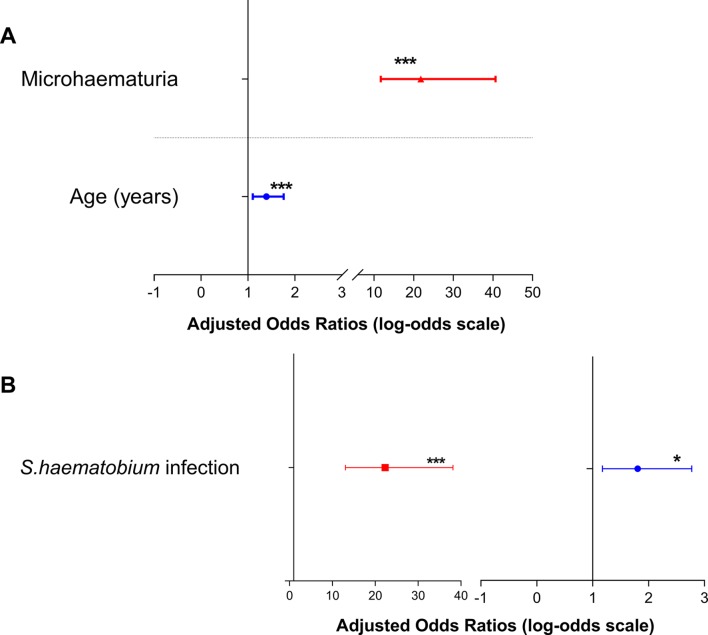
At baseline, the prevalence of infection and microhaematuria was 8.5% and 8.6%, respectively. Based on different anthropometric indices, 2.2%-8.2% of children were malnourished, 10.1% underweight and 18.0% stunted. The fraction of morbidity attributable to schistosome infection was 92% for microhaematuria, 38% for stunting and malnutrition at 9%-34%, depending on indices used. -positive children were at greater odds of presenting with microhaematuria (adjusted OR (AOR)=25.6; 95% CI 14.5 to 45.1) and stunting (AOR=1.7; 95% CI 1.1 to 2.7). Annual incidence of infection and microhaematuria was 17.4% and 20.4%, respectively. Microhaematuria occurred within 3 months of first infection and resolved in a significant number of children, 12 weeks post-praziquantel treatment, from 42.3% to 10.3%; P<0.001.
We demonstrated for the first time the incidence of schistosome infection in PSAC, along with microhaematuria, which appears within 3 months of first infection and resolves after praziquantel treatment. A proportion of stunting and malnutrition is attributable to infection. The study adds scientific evidence to the calls for inclusion of PSAC in schistosome control programmes.
近期研究表明,在血吸虫病流行地区,学龄前儿童(即5岁及以下儿童)有感染风险。然而,对于该年龄组感染和发病动态情况存在知识空白。在本研究中,我们确定了学龄前儿童首次泌尿生殖系统血吸虫感染的发病率及动态情况、发病情况和治疗情况。
招募6个月至5岁儿童并随访12个月。收集了1502名儿童的基线人口统计学、人体测量学和寄生虫学数据。通过血尿评估泌尿发病情况,使用世界卫生组织标准人体测量指数评估与生长相关的发病情况。对感染阴性的儿童每季度进行随访,以确定感染和发病发生率。
在基线时,感染和微量血尿的患病率分别为8.5%和8.6%。根据不同的人体测量指数,2.2% - 8.2%的儿童营养不良,10.1%体重不足,18.0%发育迟缓。血吸虫感染导致的发病比例,微量血尿为92%,发育迟缓为38%,营养不良为9% - 34%,具体取决于所使用的指数。感染阳性儿童出现微量血尿(调整后比值比(AOR)=25.6;95%置信区间14.5至45.1)和发育迟缓(AOR = 1.7;95%置信区间1.1至2.7)的几率更高。感染和微量血尿的年发病率分别为17.4%和20.4%。微量血尿在首次感染后3个月内出现,并且在大量儿童中,吡喹酮治疗12周后从42.3%降至10.3%;P<0.001。
我们首次证明了学龄前儿童血吸虫感染的发病率以及微量血尿情况,微量血尿在首次感染后3个月内出现,并在吡喹酮治疗后缓解。部分发育迟缓和营养不良可归因于血吸虫感染。该研究为将学龄前儿童纳入血吸虫病控制计划的呼吁增添了科学依据。