Serviço de Medicina, Hospital de Santo António, Largo Prof. Abel Salazar, 4099-001, Porto, Portugal.
Unidade de Cuidados Intensivos Polivalente, Hospital de Santo António, University of Porto, Largo Prof. Abel Salazar, 4099-001, Porto, Portugal.
BMC Infect Dis. 2018 Apr 5;18(1):161. doi: 10.1186/s12879-018-3054-4.
Severe infection is a main cause of mortality. We aim to describe risk factors for long-term mortality among inpatients with severe infection.
Prospective cohort study in a 600-bed university hospital in Portugal including all patients with severe infection admitted into intensive care, medical, surgical, hematology and nephrology wards over one-year period. The outcome of interest was 5-year mortality following infection. Variables of patient background and infectious episode were studied in association with the main outcome through multiple logistic regression. There were 1013 patients included in the study. Hospital and 5-year mortality rates were 14 and 37%, respectively.
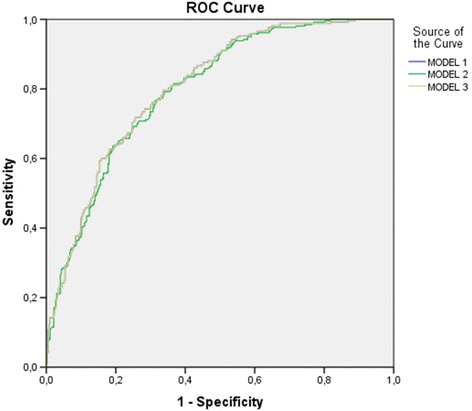
Two different models were developed (with and without acute-illness severity scores) and factors independently associated with 5-year mortality were [adjusted odds ratio (95% confidence interval)]: age = 1.03 per year (1.02-1.04), cancer = 4.36 (1.65-11.53), no comorbidities = 0.4 (0.26-0.62), Karnovsky Index < 70 = 2.25 (1.48-3.40), SAPS (Simplified Acute Physiology Score) II = 1.05 per point (1.03-1.07), positive blood cultures = 1.57 (1.01-2.44) and infection by an ESKAPE pathogen (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeroginosa and Enterobacter species) = 1.61 (1.00- 2.60); and in the second model [without SAPS II and SOFA (Sequential Organ Failure Assessment) scores]: age = 1.04 per year (1.03-1.05), cancer = 5.93 (2.26-15.51), chronic haematologic disease = 2.37 (1.14-4.93), no comorbidities = 0.45 (0.29-0.69), Karnovsky Index< 70 = 2.32 (1.54- 3.50), septic shock [reference is infection without SIRS (Systemic Inflammatory Response Syndrome)] = 3.77 (1.80-7.89) and infection by an ESKAPE pathogen = 1.61 (1.00-2.60). Both models presented a good discrimination power with an AU-ROC curve (95% CI) of 0.81 (0.77-0.84) for model 1 and 0.80 (0.76-0.83) for model 2. If only patients that survived hospital admission are included in the model, variables retained are: age = 1.03 per year (1.02-1.05), cancer = 4.69 (1.71-12.83), chronic respiratory disease = 2.27 (1.09-4.69), diabetes mellitus = 1.65 (1.06-2.56), Karnovsky Index < 70 = 2.50 (1.63-3.83) and positive blood cultures = 1.66 (1.04-2.64) with an AU-ROC curve of 0.77 (0.73-0.81).
Age, previous comorbidities, and functional status and infection by an ESKAPE pathogen were consistently associated with long-term prognosis. This information may help in the discussion of individual prognosis and clinical decision-making.
严重感染是导致死亡的主要原因。本研究旨在描述重症感染患者长期死亡的危险因素。
这是一项在葡萄牙一家拥有 600 张床位的大学医院进行的前瞻性队列研究,纳入了重症监护病房、内科、外科、血液科和肾病科病房中所有严重感染患者。感染后 5 年死亡率是研究的主要终点。通过多因素逻辑回归分析患者背景和感染情况与主要结局的关系。共纳入 1013 例患者,医院和 5 年死亡率分别为 14%和 37%。
建立了两个不同的模型(有和没有急性疾病严重程度评分),与 5 年死亡率相关的独立因素为[校正比值比(95%置信区间)]:年龄每年增加 1.03(1.02-1.04),癌症 4.36(1.65-11.53),无合并症 0.4(0.26-0.62),卡诺夫斯基指数<70 2.25(1.48-3.40),简化急性生理学评分 II 每增加 1 分 1.05(1.03-1.07),血培养阳性 1.57(1.01-2.44)和感染 ESKAPE 病原体(屎肠球菌、金黄色葡萄球菌、肺炎克雷伯菌、鲍曼不动杆菌、铜绿假单胞菌和肠杆菌属)1.61(1.00-2.60);在第二个模型中(无 SAPS II 和 SOFA 评分):年龄每年增加 1.04(1.03-1.05),癌症 5.93(2.26-15.51),慢性血液系统疾病 2.37(1.14-4.93),无合并症 0.45(0.29-0.69),卡诺夫斯基指数<70 2.32(1.54-3.50),感染性休克[参考为无全身炎症反应综合征的感染]3.77(1.80-7.89)和感染 ESKAPE 病原体 1.61(1.00-2.60)。两个模型均具有良好的区分能力,模型 1 的 AU-ROC 曲线(95%CI)为 0.81(0.77-0.84),模型 2 为 0.80(0.76-0.83)。如果仅纳入存活出院患者的模型,保留的变量为:年龄每年增加 1.03(1.02-1.05),癌症 4.69(1.71-12.83),慢性呼吸系统疾病 2.27(1.09-4.69),糖尿病 1.65(1.06-2.56),卡诺夫斯基指数<70 2.50(1.63-3.83)和血培养阳性 1.66(1.04-2.64),AU-ROC 曲线为 0.77(0.73-0.81)。
年龄、既往合并症、功能状态和感染 ESKAPE 病原体与长期预后相关。这些信息可能有助于讨论个体预后和临床决策。