Fanaroff Alexander C, Li Shuang, Webb Laura E, Miller Vincent, Navar Ann Marie, Peterson Eric D, Wang Tracy Y
Department of Medicine (A.C.F., A.M.N., E.D.P., T.Y.W.) and Duke Clinical Research Institute (A.C.F., A.M.N., E.D.P., T.Y.W., S.L., L.E.W., V.M.,), Duke University Medical Center, Durham, NC.
Circ Cardiovasc Qual Outcomes. 2018 Apr;11(4):e004675. doi: 10.1161/CIRCOUTCOMES.118.004675.
Patient participation in clinical research is low, in part because of the length and complexity of the informed consent process. Video informed consent may enhance the appeal of research and help break down barriers to participation.
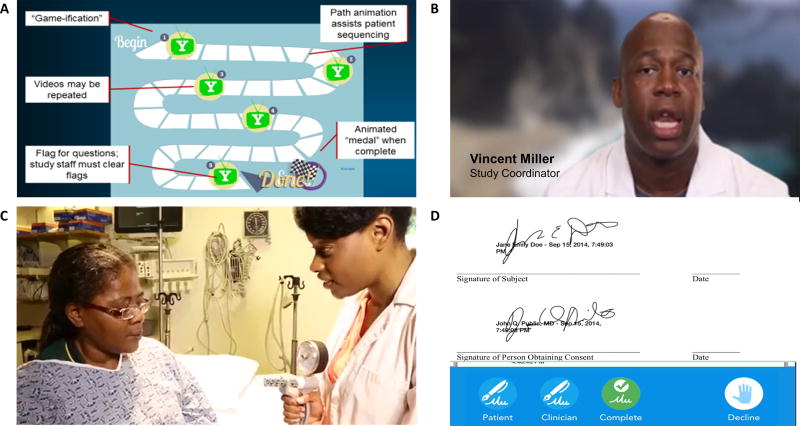
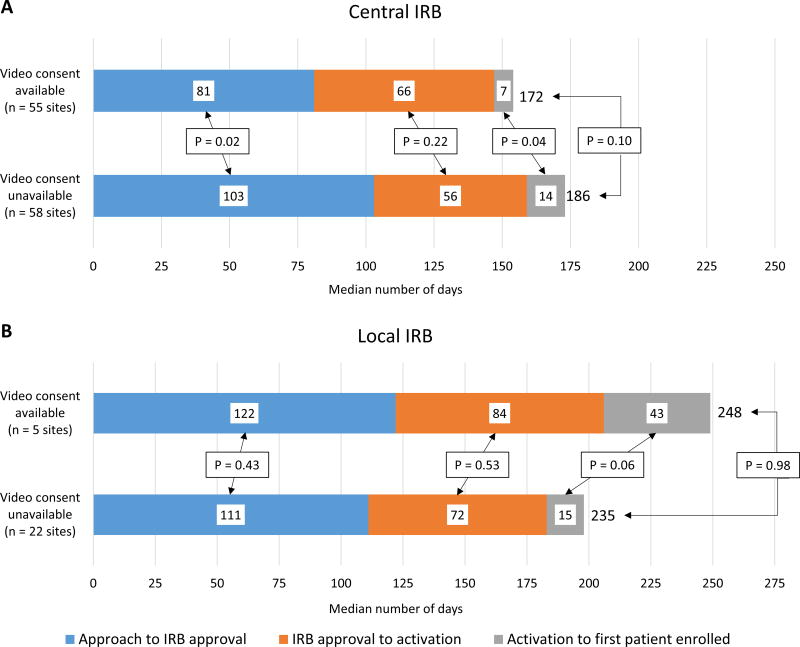
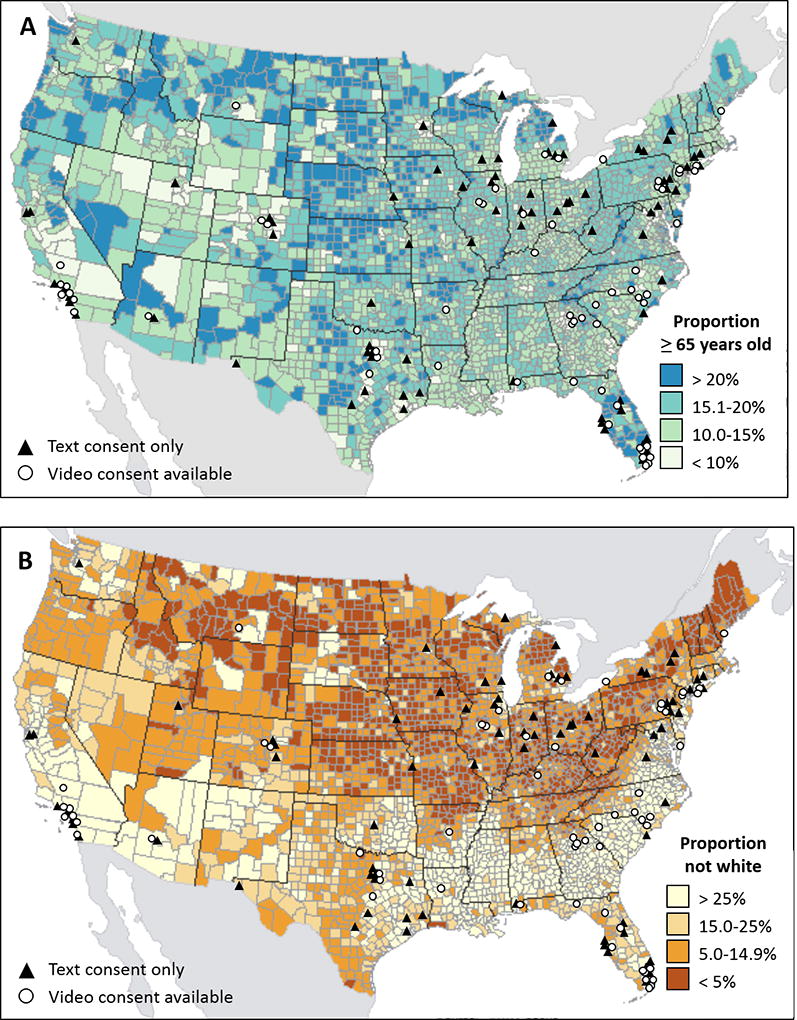
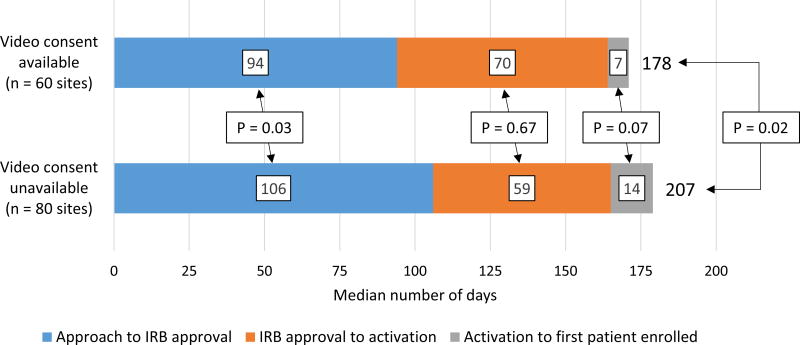
The PALM study (Patient and Provider Assessment of Lipid Management) enrolled 7904 patients at cardiology, endocrinology, and primary care clinics across the United States to evaluate cholesterol management practices. Of 153 participating clinics, 67 (43.8%) secured institutional review board approval to use a tablet-based video informed consent tool that patients could select to navigate through the informed consent process instead of traditional text-based informed consent. At sites without institutional review board approval of video consent, all patients read a text-based informed consent document. Site activation times and enrollment volumes, as well as characteristics of enrolled patients, were compared between sites with and without video consent capability. Sites with video consent capability more often used a central institutional review board (89.6% versus 73.3%), were more often rural (16.7% versus 3.8%), and tended to have fewer providers. Compared with sites without video consent capability, sites with video consent capability had shorter times from site approach to first patient enrollment (median 178 versus 207 days; =0.02). Sites with video consent capability enrolled similar numbers of patients as sites without video consent capability (=0.48) but enrolled a greater proportion of patients who were ≥75 years old (27.5% versus 23.6%; <0.001) and nonwhite (17.7% versus 14.2%; <0.001).
In this observational study of recruitment in a multicenter registry, sites approved for video consent use enrolled the same number of patients as sites with only traditional text-based informed consent but had faster speed to first patient enrolled and more often enrolled older and nonwhite patients. Future randomized trials are needed to assess the impact of video consent on enrollment mechanics and demographics.
URL: https://www.clinicaltrials.gov. Unique identifier: NCT02341664.
患者参与临床研究的比例较低,部分原因是知情同意过程的长度和复杂性。视频知情同意可能会提高研究的吸引力,并有助于消除参与的障碍。
PALM研究(患者和提供者对血脂管理的评估)在美国各地的心脏病学、内分泌学和初级保健诊所招募了7904名患者,以评估胆固醇管理实践。在153家参与的诊所中,67家(43.8%)获得了机构审查委员会的批准,使用基于平板电脑的视频知情同意工具,患者可以选择通过该工具浏览知情同意过程,而不是传统的基于文本的知情同意。在没有获得机构审查委员会视频同意批准的地点,所有患者阅读基于文本的知情同意文件。比较了有和没有视频同意能力的地点之间的地点激活时间和入组人数,以及入组患者的特征。有视频同意能力的地点更常使用中央机构审查委员会(89.6%对73.3%),更常位于农村地区(16.7%对3.8%),且提供者往往较少。与没有视频同意能力的地点相比,有视频同意能力的地点从接触地点到首次患者入组的时间更短(中位数为178天对207天;P=0.02)。有视频同意能力的地点入组患者数量与没有视频同意能力的地点相似(P=0.48),但≥75岁患者(27.5%对23.6%;P<0.001)和非白人患者(17.7%对14.2%;P<0.001)的入组比例更高。
在这项多中心注册研究的招募观察性研究中,被批准使用视频同意的地点入组患者数量与仅使用传统基于文本的知情同意的地点相同,但首次患者入组速度更快,且更常入组老年和非白人患者。未来需要进行随机试验,以评估视频同意对入组机制和人口统计学的影响。