Mwanza Jean-Claude, Lee Gary, Budenz Donald L, Warren Joshua L, Wall Michael, Artes Paul H, Callan Thomas M, Flanagan John G
Department of Ophthalmology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Research and Development, Carl Zeiss Meditec, Inc., Dublin, CA, USA.
Transl Vis Sci Technol. 2018 Apr 3;7(2):16. doi: 10.1167/tvst.7.2.16. eCollection 2018 Apr.
To independently validate the performance of the University of North Carolina Optical Coherence Tomography (UNC OCT) Index in diagnosing and predicting early glaucoma.
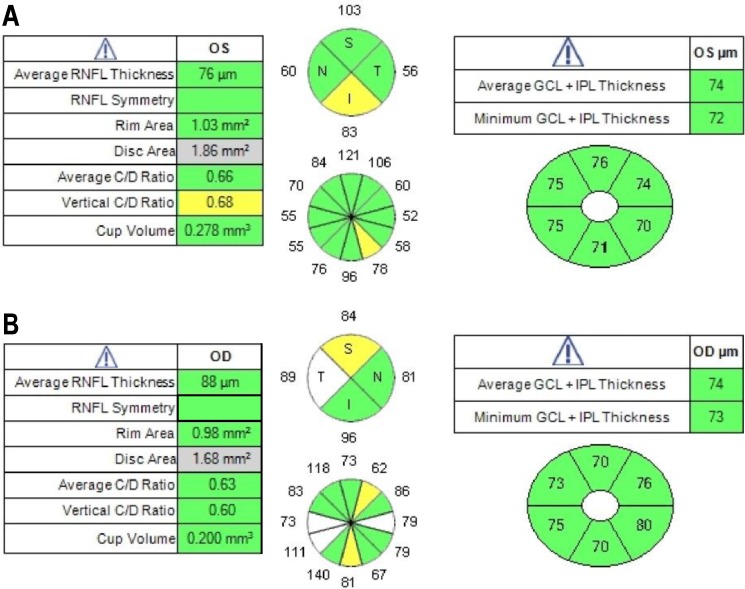
Data of 118 normal subjects (118 eyes) and 96 subjects (96 eyes) with early glaucoma defined as visual field mean deviation (MD) greater than -4 decibels (dB), aged 40 to 80 years, and who were enrolled in the Full-Threshold Testing Size III, V, VI comparison study were used in this study. CIRRUS OCT average and quadrants' retinal nerve fiber layer (RNFL); optic disc vertical cup-to-disc ratio (VCDR), cup-to-disc area ratio, and rim area; and average, minimum, and six sectoral ganglion cell-inner plexiform layer (GCIPL) measurements were run through the UNC OCT Index algorithm. Area under the receiver operating characteristic curve (AUC) and sensitivities at 95% and 99% specificity were calculated and compared between single parameters and the UNC OCT Index.
Mean age was 60.1 ± 11.0 years for normal subjects and 66.5 ± 8.1 years for glaucoma patients ( < 0.001). MD was 0.29 ± 1.04 dB and -1.30 ± 1.35 dB in normal and glaucomatous eyes ( < 0.001), respectively. The AUC of the UNC OCT Index was 0.96. The best single metrics when compared to the UNC OCT Index were VCDR (0.93, = 0.054), average RNFL (0.92, = 0.014), and minimum GCIPL (0.91, = 0.009). The sensitivities at 95% and 99% specificity were 85.4% and 76.0% (UNC OCT Index), 71.9% and 62.5% (VCDR, all < 0.001), 64.6% and 53.1% (average RNFL, all < 0.001), and 66.7% and 58.3% (minimum GCIPL, all < 0.001), respectively.
The findings confirm that the UNC OCT Index may provide improved diagnostic perforce over that of single OCT parameters and may be a good tool for detection of early glaucoma.
The UNC OCT Index algorithm may be incorporated easily into routine clinical practice and be useful for detecting early glaucoma.
独立验证北卡罗来纳大学光学相干断层扫描(UNC OCT)指数在诊断和预测早期青光眼方面的性能。
本研究使用了118名正常受试者(118只眼)和96名早期青光眼受试者(96只眼)的数据,这些受试者年龄在40至80岁之间,早期青光眼定义为视野平均偏差(MD)大于-4分贝(dB),并参与了全阈值测试大小III、V、VI比较研究。对CIRRUS OCT平均和象限视网膜神经纤维层(RNFL);视盘垂直杯盘比(VCDR)、杯盘面积比和边缘面积;以及平均、最小和六个扇形神经节细胞-内丛状层(GCIPL)测量值进行UNC OCT指数算法运算。计算并比较单参数与UNC OCT指数之间的受试者操作特征曲线下面积(AUC)以及95%和99%特异性时的敏感性。
正常受试者的平均年龄为60.1±11.0岁,青光眼患者为66.5±8.1岁(P<0.001)。正常眼和青光眼眼中的MD分别为0.29±1.04 dB和-1.30±1.35 dB(P<0.001)。UNC OCT指数的AUC为0.96。与UNC OCT指数相比,最佳的单一指标是VCDR(0.93,P = 0.054)、平均RNFL(0.92,P = 0.014)和最小GCIPL(0.91,P = 0.009)。95%和99%特异性时的敏感性分别为85.4%和76.0%(UNC OCT指数)、71.9%和62.5%(VCDR,均P<0.001)、64.6%和53.1%(平均RNFL,均P<0.001)以及66.7%和58.3%(最小GCIPL,均P<0.001)。
研究结果证实,UNC OCT指数在诊断效能上可能优于单一OCT参数,可能是检测早期青光眼的良好工具。
UNC OCT指数算法可轻松纳入常规临床实践,有助于检测早期青光眼。