Departments of Obstetrics and Gynecology and Psychiatry, Virginia Commonwealth University, Richmond, Virginia; the Department of Obstetrics, Gynecology & Reproductive Sciences, Magee-Womens Research Institute, University of Pittsburgh, Pittsburgh, Pennsylvania; the Department of Obstetrics & Gynecology, Psychiatry & Human Behavior, Thomas Jefferson University, Philadelphia, Pennsylvania; the Department of Obstetrics, Gynecology, and Women's Health, University of Hawaii, Honolulu, Hawaii; the Department of Obstetrics and Gynecology, Northwestern University, Chicago, Illinois; the Department Obstetrics and Gynecology, University of North Carolina, Chapel Hill, Chapel Hill, North Carolina; and the Department of Obstetrics, Gynecology & Reproductive Services, University of Vermont, Burlington, Vermont.
Obstet Gynecol. 2018 May;131(5):803-814. doi: 10.1097/AOG.0000000000002562.
To systematically review maternal and neonatal outcomes associated with opioid detoxification during pregnancy.
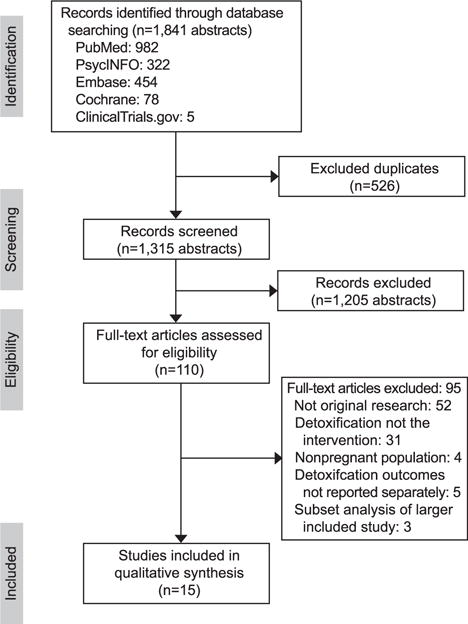
PubMed, PsycINFO, EMBASE, Cochrane, and ClinicalTrials.gov databases were searched from January 1, 1966, to September 1, 2016.
English-language studies that reported outcomes associated with opioid detoxification among pregnant women with opioid use disorder were included. Nonoriginal research articles (case reports, editorials, reviews) and studies that failed to report outcomes for detoxification participants were excluded. Bias was assessed using the Cochrane Collaboration's tool for assessing risk of bias and quality was assessed using the U.S. Preventive Service Task Force Quality of Evidence scale.
TABULATION, INTEGRATION, AND RESULTS: Of 1,315 unique abstracts identified, 15 met criteria for inclusion and included 1,997 participants, of whom 1,126 underwent detoxification. Study quality ranged from fair to poor as a result of the lack of a randomized control or comparison arm and high risk of bias across all studies. Only nine studies had a comparison arm. Detoxification completion (9-100%) and illicit drug relapse (0-100%) rates varied widely across studies depending on whether data from participants who did not complete detoxification or who were lost to follow-up were included in analyses. The reported rate of fetal loss was similar among women who did (14 [1.2%]) and did not undergo detoxification (17 [2.0%]).
Evidence does not support detoxification as a recommended treatment intervention as a result of low detoxification completion rates, high rates of relapse, and limited data regarding the effect of detoxification on maternal and neonatal outcomes beyond delivery.
系统评价与妊娠期间阿片类药物戒断相关的母婴结局。
从 1966 年 1 月 1 日至 2016 年 9 月 1 日,检索了 PubMed、PsycINFO、EMBASE、Cochrane 和 ClinicalTrials.gov 数据库。
纳入了报告阿片类药物使用障碍孕妇接受阿片类药物戒断相关结局的英语语言研究。排除非原始研究文章(病例报告、社论、综述)和未报告戒断参与者结局的研究。使用 Cochrane 协作组评估偏倚的工具评估偏倚风险,使用美国预防服务工作组质量证据量表评估质量。
从 1315 篇独特的摘要中,有 15 篇符合纳入标准,共纳入 1997 名参与者,其中 1126 名接受了戒断。由于缺乏随机对照或比较组以及所有研究的偏倚风险高,研究质量从低到高。只有 9 项研究有比较组。戒断完成率(9-100%)和非法药物复吸率(0-100%)因是否将未完成戒断或失访的参与者的数据纳入分析而在研究间差异很大。接受戒断和未接受戒断的女性胎儿丢失率相似(分别为 14 [1.2%]和 17 [2.0%])。
由于戒断完成率低、复吸率高,以及关于戒断对分娩后母婴结局影响的数据有限,证据不支持将戒断作为推荐的治疗干预措施。