Ireen Santhia, Raihan Mohammad Jyoti, Choudhury Nuzhat, Islam M Munirul, Hossain Md Iqbal, Islam Ziaul, Rahman S M Mustafizur, Ahmed Tahmeed
Nutrition and Clinical Services Division, International Centre for Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh.
Health Systems and Population Studies Division, International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh.
BMC Health Serv Res. 2018 Apr 10;18(1):256. doi: 10.1186/s12913-018-3087-9.
Severe acute malnutrition (SAM) in children is the most serious form of malnutrition and is associated with very high rates of morbidity and mortality. For sustainable SAM management, United Nations recommends integration of community based management of acute malnutrition (CMAM) into the health system. The objective of the study was to assess the preparedness of the health system to implement CMAM in Bangladesh.
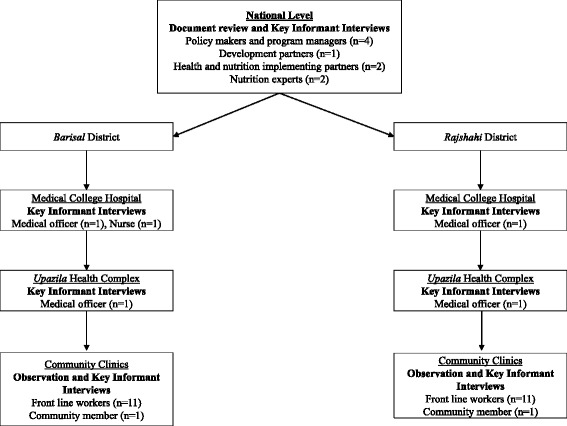
The assessment was undertaken during January to May 2014 by conducting document review, key informant interviews, and direct observation. A total of 38 key informant interviews were conducted among government policy makers and program managers (n = 4), nutrition experts (n = 2), health and nutrition implementing partners (n = 2), development partner (n = 1), government health system staff (n = 5), government front line field workers (n = 22), and community members (n = 2). The assessment was based on: workforce, service delivery, financing, governance, information system, medical supplies, and the broad socio-political context.
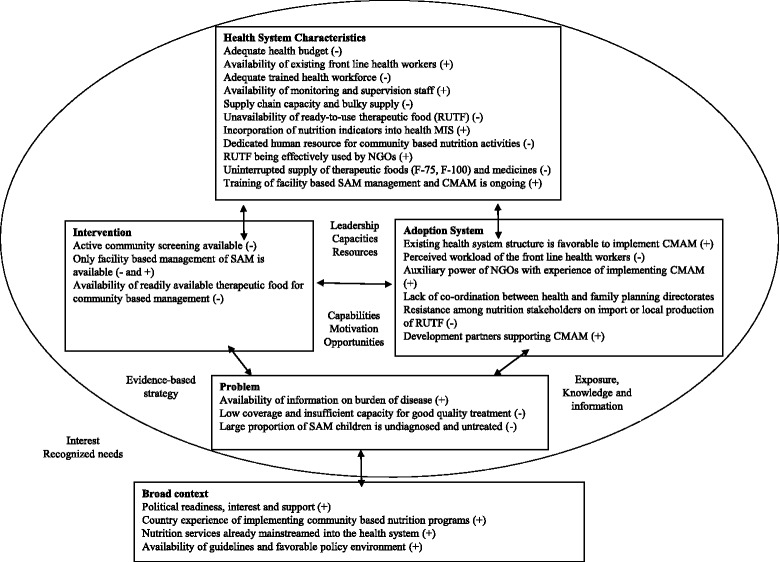
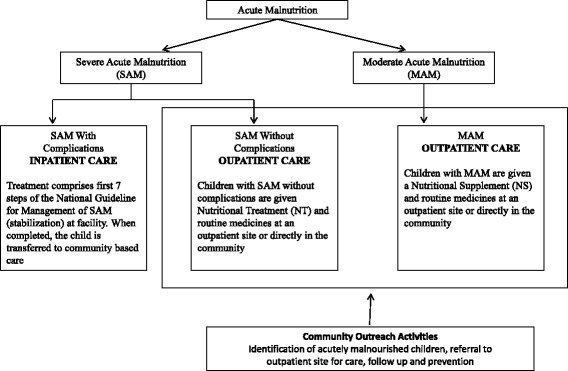
The government of Bangladesh has developed inpatient and outpatient guidelines for the management of SAM. There are cadres of community health workers of government and non-government actors who can be adequately trained to conduct CMAM. Inpatient management of SAM is available in 288 facilities across the country. However, only 2.7% doctors and 3.3% auxiliary staff are trained on facility based management of SAM. In functional facilities, uninterrupted supply of medicines and therapeutic diet are not available. There is resistance and disagreement among nutrition stakeholders regarding import or local production of ready-to-use therapeutic food (RUTF). Nutrition coordination is fragile and there is no functional supra-ministerial coordination platform for multi-sectoral and multi-stakeholder nutrition.
There is an enabling environment for CMAM intervention in Bangladesh although health system strengthening is needed considering the barriers that have been identified. Training of facility based health staff, government community workers, and ensuring uninterrupted supply of medicines and logistics to the functional facilities should be the immediate priorities. Availability of ready-to-use therapeutic food (RUTF) is a critical component of CMAM and government should promote in-country production of RUTF for effective integration of CMAM into the health system in Bangladesh.
儿童严重急性营养不良(SAM)是最严重的营养不良形式,与极高的发病率和死亡率相关。为实现可持续的SAM管理,联合国建议将基于社区的急性营养不良管理(CMAM)纳入卫生系统。本研究的目的是评估孟加拉国卫生系统实施CMAM的准备情况。
2014年1月至5月期间,通过文献回顾、关键信息人访谈和直接观察进行评估。共对政府政策制定者和项目管理人员(n = 4)、营养专家(n = 2)、卫生和营养实施伙伴(n = 2)、发展伙伴(n = 1)、政府卫生系统工作人员(n = 5)、政府一线现场工作人员(n = 22)和社区成员(n = 2)进行了38次关键信息人访谈。评估基于:劳动力、服务提供、融资、治理、信息系统、医疗用品以及广泛的社会政治背景。
孟加拉国政府已制定了SAM管理的住院和门诊指南。政府和非政府行为体有社区卫生工作者队伍,可对其进行充分培训以开展CMAM。全国有288家机构提供SAM的住院治疗。然而,只有2.7%的医生和3.3%的辅助人员接受过基于机构的SAM管理培训。在正常运转的机构中,药品和治疗性饮食无法持续供应。营养利益相关者在即食治疗食品(RUTF)的进口或本地生产方面存在抵触和分歧。营养协调薄弱,没有一个为多部门和多利益攸关方营养问题设立的有效跨部门协调平台。
孟加拉国存在开展CMAM干预的有利环境,不过鉴于已发现的障碍,仍需加强卫生系统。当务之急是培训基于机构的卫生工作人员和政府社区工作者,并确保向正常运转的机构持续供应药品和后勤物资。即食治疗食品(RUTF)的供应是CMAM的关键组成部分,政府应推动在国内生产RUTF,以便将CMAM有效纳入孟加拉国的卫生系统。