Department of Medicine, Vanderbilt University Medical Center, 1161 21st Avenue South, T3113 MCN, Nashville, TN, 37232, USA.
Department of Biomedical Informatics, Vanderbilt University Medical Center, Nashville, TN, USA.
Arthritis Res Ther. 2018 Apr 10;20(1):69. doi: 10.1186/s13075-018-1561-8.
African Americans with systemic lupus erythematosus (SLE) have increased renal disease compared to Caucasians, but differences in other comorbidities have not been well-described. We used an electronic health record (EHR) technique to test for differences in comorbidities in African Americans compared to Caucasians with SLE.
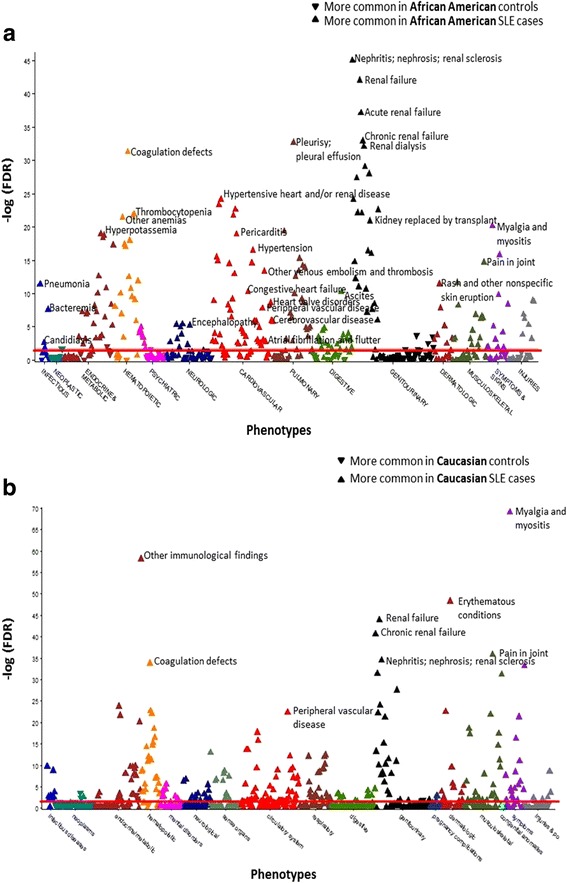
We used a de-identified EHR with 2.8 million subjects to identify SLE cases using a validated algorithm. We performed phenome-wide association studies (PheWAS) comparing African American to Caucasian SLE cases and African American SLE cases to matched non-SLE controls. Controls were age, sex, and race matched to SLE cases. For multiple testing, a false discovery rate (FDR) p value of 0.05 was used.
We identified 270 African Americans and 715 Caucasians with SLE and 1425 matched African American controls. Compared to Caucasians with SLE adjusting for age and sex, African Americans with SLE had more comorbidities in every organ system. The most striking included hypertension odds ratio (OR) = 4.25, FDR p = 5.49 × 10; renal dialysis OR = 10.90, FDR p = 8.75 × 10; and pneumonia OR = 3.57, FDR p = 2.32 × 10. Compared to the African American matched controls without SLE, African Americans with SLE were more likely to have comorbidities in every organ system. The most significant codes were renal and cardiac, and included renal failure (OR = 9.55, FDR p = 2.26 × 10) and hypertensive heart and renal disease (OR = 8.08, FDR p = 1.78 × 10). Adjusting for race, age, and sex in a model including both African American and Caucasian SLE cases and controls, SLE was independently associated with renal, cardiovascular, and infectious diseases (all p < 0.01).
African Americans with SLE have an increased comorbidity burden compared to Caucasians with SLE and matched controls. This increase in comorbidities in African Americans with SLE highlights the need to monitor for cardiovascular and infectious complications.
与高加索人相比,患有系统性红斑狼疮(SLE)的非裔美国人肾脏疾病的发生率更高,但其他合并症的差异尚未得到很好的描述。我们使用电子病历(EHR)技术来测试非裔美国人与患有 SLE 的高加索人之间合并症的差异。
我们使用一个包含 280 万受试者的去识别 EHR 来使用经过验证的算法识别 SLE 病例。我们进行了表型全基因组关联研究(PheWAS),比较了非裔美国人和高加索人 SLE 病例以及非裔美国 SLE 病例与匹配的非 SLE 对照之间的差异。对照与 SLE 病例在年龄、性别和种族上相匹配。对于多次检验,使用错误发现率(FDR)p 值为 0.05。
我们确定了 270 名非裔美国人和 715 名高加索人患有 SLE,以及 1425 名匹配的非裔美国对照。与调整年龄和性别后患有 SLE 的高加索人相比,患有 SLE 的非裔美国人在每个器官系统中都有更多的合并症。最显著的包括高血压比值比(OR)=4.25,FDR p =5.49×10;肾透析 OR =10.90,FDR p =8.75×10;和肺炎 OR =3.57,FDR p =2.32×10。与没有 SLE 的非裔美国匹配对照相比,患有 SLE 的非裔美国人在每个器官系统中更有可能患有合并症。最显著的代码是肾脏和心脏的,包括肾衰竭(OR =9.55,FDR p =2.26×10)和高血压性心脏和肾脏疾病(OR =8.08,FDR p =1.78×10)。在一个包括非裔美国人和高加索人 SLE 病例和对照的模型中,在调整种族、年龄和性别后,SLE 与肾脏、心血管和传染病独立相关(均 p<0.01)。
与患有 SLE 的高加索人相比,患有 SLE 的非裔美国人的合并症负担更高,与匹配的对照相比也是如此。患有 SLE 的非裔美国人合并症的增加突出表明需要监测心血管和感染性并发症。