Rees Clare M, Hall Nigel J, Fleming Paul, Eaton Simon
UCL Great Ormond Street Institute of Child Health and Great Ormond Street Hospital for Children NHS Trust, London, UK.
Department of Paediatric Surgery and Urology, Faculty of Medicine, University of Southampton, Southampton, UK.
BMJ Paediatr Open. 2017 Nov 1;1(1):e000066. doi: 10.1136/bmjpo-2017-000066. eCollection 2017.
Probiotic administration to preterm infants has the potential to prevent necrotising enterocolitis (NEC). Data from randomised controlled trials (RCT) are conflicting but meta-analyses seem to support this intervention. To date, these analyses have not focused on surgical NEC. We aimed to determine the effect of probiotic administration to preterm infants on prevention of surgical NEC.
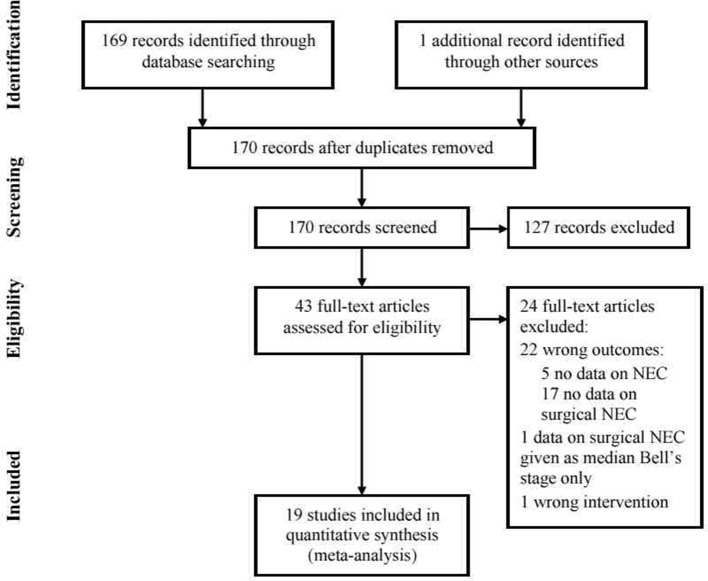
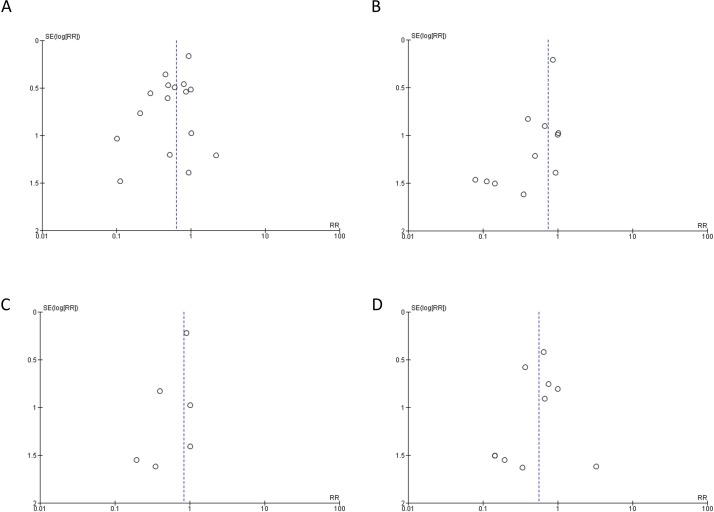
A systematic review of RCTs of probiotic administration to preterm infants was performed. Studies were included if RCT outcomes included any of (1) Bell's stage 3 NEC; (2) surgery for NEC; and (3) deaths attributable to NEC. Article selection and data extraction were performed independently by two authors; conflicts were adjudicated by a third author. Data were meta-analysed using Review Manager V.5.3. A random effects model was decided on a priori because of the heterogeneity of study design; data are risk ratio (RR) with 95% CI.
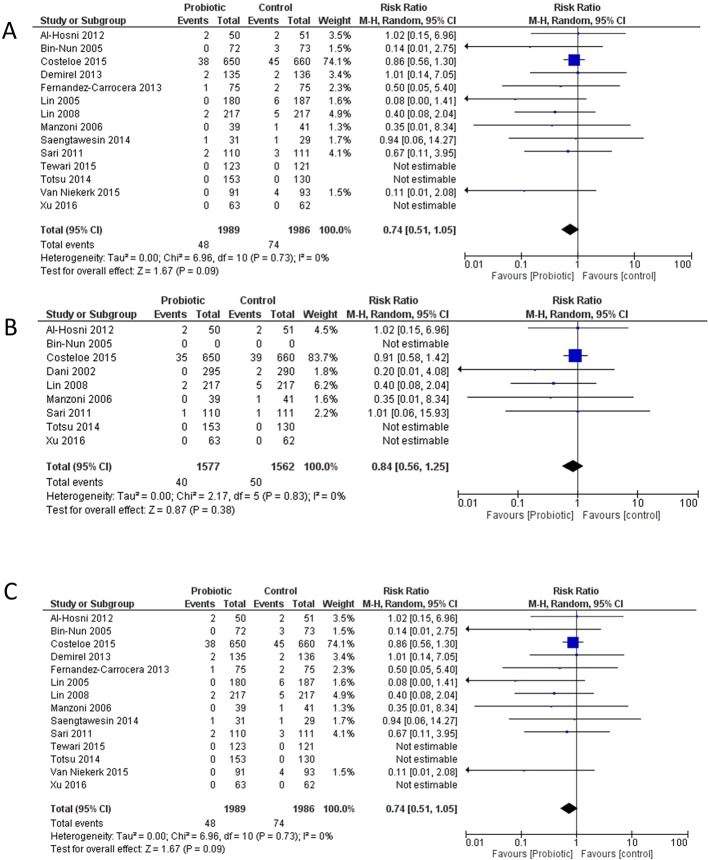
Thirty-five RCTs reported NEC as an outcome. Seventeen reported surgical NEC; all RCTs were included. A variety of probiotic products was administered across studies. Description of surgical NEC in most studies was poor. Only 6/16 specifically reported incidence of surgery for NEC, 12/17 Bell's stage 3 and 13/17 NEC-associated mortality. Although there was a trend towards probiotic administration reducing stage 3 NEC, this was not significant (RR 0.74 (0.52-1.05), p=0.09). There was no effect of probiotics on the RR of surgery for NEC (RR 0.84 (0.56-1.25), p=0.38). Probiotics did, however, reduce the risk of NEC-associated mortality (RR 0.56 (0.34-0.93), p=0.03).
Despite 35 RCTs on probiotic prevention of NEC, evidence for prevention of surgical NEC is not strong, partly due to poor reporting. In studies included in this meta-analysis, probiotic administration was associated with a reduction in NEC-related mortality.
对早产儿使用益生菌有可能预防坏死性小肠结肠炎(NEC)。随机对照试验(RCT)的数据存在冲突,但荟萃分析似乎支持这种干预措施。迄今为止,这些分析尚未聚焦于外科坏死性小肠结肠炎。我们旨在确定对早产儿使用益生菌预防外科坏死性小肠结肠炎的效果。
对给早产儿使用益生菌的随机对照试验进行系统评价。如果随机对照试验的结果包括以下任何一项,则纳入研究:(1)贝尔3期坏死性小肠结肠炎;(2)坏死性小肠结肠炎手术;(3)因坏死性小肠结肠炎导致的死亡。文章筛选和数据提取由两位作者独立进行;分歧由第三位作者裁决。使用Review Manager V.5.3对数据进行荟萃分析。由于研究设计的异质性,事先决定采用随机效应模型;数据为风险比(RR)及95%置信区间。
35项随机对照试验将坏死性小肠结肠炎作为一项结果进行了报告。17项报告了外科坏死性小肠结肠炎;所有随机对照试验均被纳入。各项研究中使用了多种益生菌产品。大多数研究对外科坏死性小肠结肠炎的描述欠佳。只有6/16具体报告了坏死性小肠结肠炎手术的发生率,12/17报告了贝尔3期,13/17报告了坏死性小肠结肠炎相关死亡率。尽管使用益生菌有降低3期坏死性小肠结肠炎的趋势,但并不显著(RR 0.74(0.52 - 1.05),p = 0.09)。益生菌对坏死性小肠结肠炎手术的风险比没有影响(RR 0.84(0.56 - 1.25),p = 0.38)。然而,益生菌确实降低了坏死性小肠结肠炎相关死亡率的风险(RR 0.56(0.34 - 0.93),p = 0.03)。
尽管有35项关于益生菌预防坏死性小肠结肠炎的随机对照试验,但预防外科坏死性小肠结肠炎的证据并不充分,部分原因是报告不佳。在这项荟萃分析纳入的研究中,使用益生菌与坏死性小肠结肠炎相关死亡率的降低有关。