Gray Amy Zigrida, Morpeth Melinda, Duke Trevor, Peel David, Winter Christian, Satvady Manivanh, Sisouk Kongkham, Prasithideth Bouasengnignom, Detleuxay Khamsay
Department of Paediatrics, Centre for International Child Health, The University of Melbourne, Parkville, Victoria, Australia.
The Royal Children's Hospital, Melbourne Australia, Parkville, Victoria, Australia.
BMJ Paediatr Open. 2017 Aug 31;1(1):e000083. doi: 10.1136/bmjpo-2017-000083. eCollection 2017.
Hypoxaemia is a common and potentially fatal complication of many childhood, newborn and maternal conditions but often not well recognised or managed in settings where resources are limited. Oxygen itself is often inaccessible due to cost or logistics. This paper describes implementation of oxygen systems in Lao district hospitals, clinical outcomes after 24 months and equipment outcomes after 40 months postimplementation.
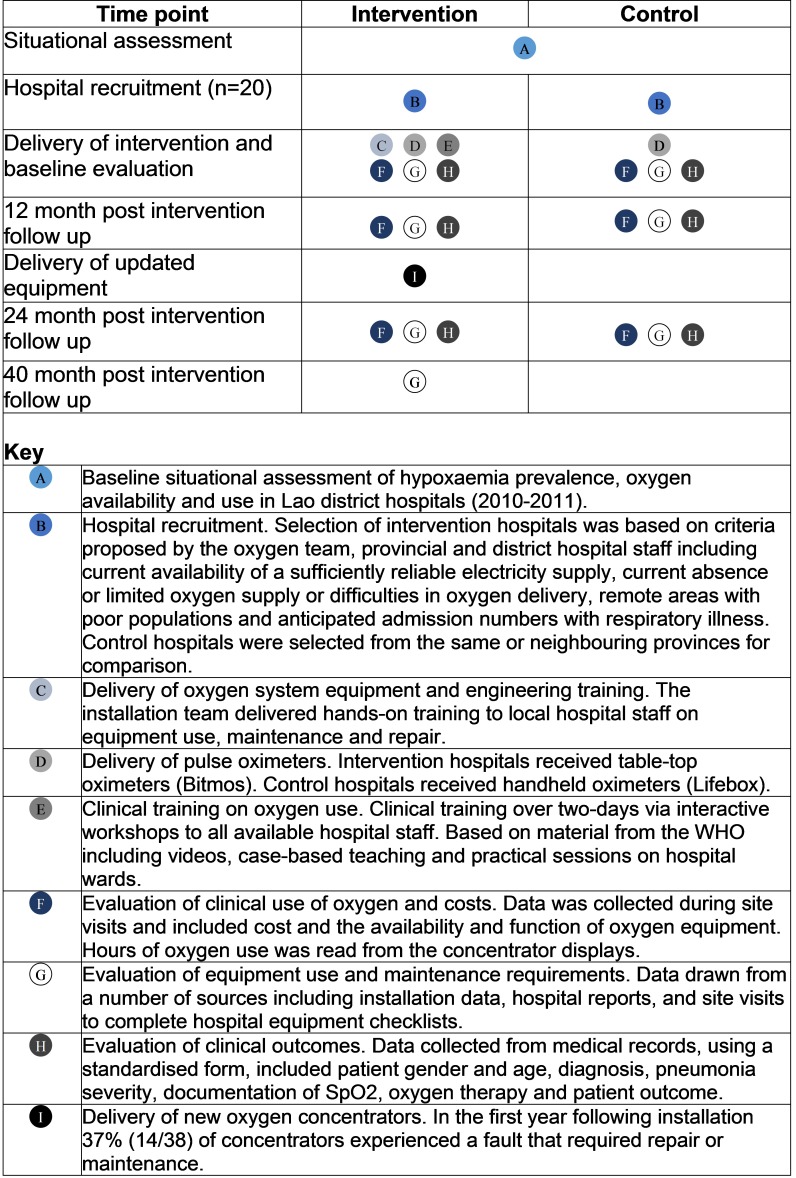
A prospective field trial was conducted in 20 district hospitals, including 10 intervention hospitals that received oxygen concentrators and 10 control hospitals. Equipment outcomes were evaluated at baseline, 12, 24 and 40 months. Clinical outcomes of children under 5 years of age with pneumonia were evaluated using a before-and-after controlled study design with information retrospectively collected from medical records.
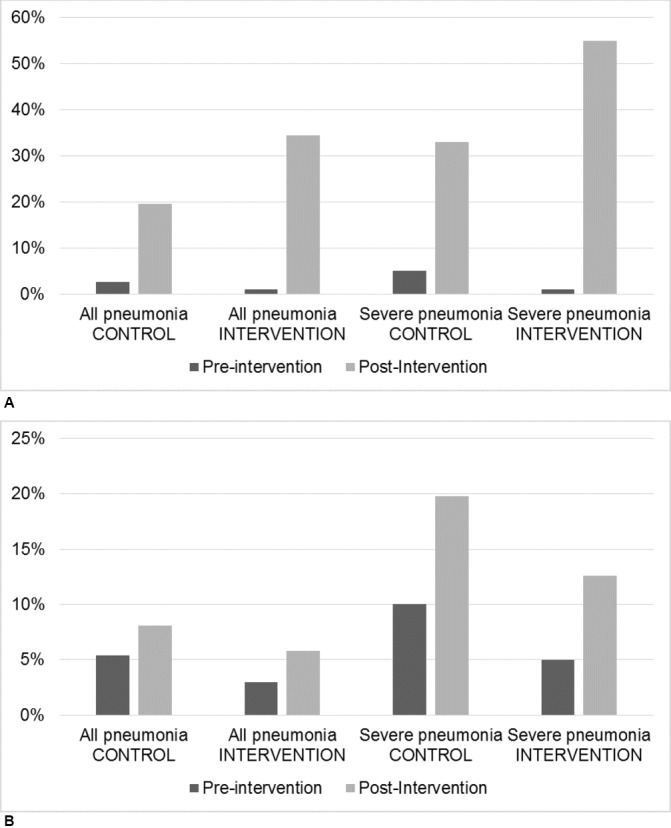
Fourteen (37%), 7 (18%) and 12 (34%) of 38 concentrators required repair at 12, 24 and 40 months, respectively. The proportion of children discharged well increased in intervention (90% (641/712) to 95.2% (658/691)) and control hospitals (87.1% (621/713) to 92.1% (588/606)). In intervention hospitals, case fatality rates for childhood pneumonia fell from 2.7% (19/712) preintervention to 0.80% (6/691) postintervention with no change in control hospitals (1.7% (12/713) preintervention and 2.3% (14/606) postintervention).
Medium-term sustainability of oxygen concentrators in hospitals accompanied by reduced case fatality for childhood pneumonia has been demonstrated in Lao PDR. Significant local engineering capacity to address multiple causes of equipment malfunction was critical. The ongoing requirements and fragile structures within the health system remain major risks to long-term sustainability.
低氧血症是许多儿童、新生儿及孕产妇疾病常见且可能致命的并发症,但在资源有限的环境中往往未得到充分认识和妥善处理。由于成本或后勤问题,氧气本身常常难以获取。本文描述了老挝地区医院氧气系统的实施情况、实施24个月后的临床结果以及实施40个月后的设备情况。
在20家地区医院进行了一项前瞻性现场试验,其中10家为干预医院,接收了制氧机,另外10家为对照医院。在基线、12个月、24个月和40个月时评估设备情况。采用前后对照研究设计,通过回顾病历收集信息,评估5岁以下肺炎儿童的临床结果。
38台制氧机中,分别有14台(37%)、7台(18%)和12台(34%)在12个月、24个月和40个月时需要维修。干预医院(从90%(641/712)增至95.2%(658/691))和对照医院(从87.1%(621/713)增至92.1%(588/606))中康复出院儿童的比例均有所增加。在干预医院,儿童肺炎病死率从干预前的2.7%(19/712)降至干预后的0.80%(6/691),对照医院则无变化(干预前为1.7%(12/713),干预后为2.3%(14/606))。
老挝已证明医院制氧机具有中期可持续性,同时儿童肺炎病死率降低。具备解决设备故障多种原因的重要本地工程能力至关重要。卫生系统内持续的需求和脆弱的结构仍是长期可持续性的主要风险。