Salmazo Péricles Sidnei, Bazan Silméia Garcia Zanati, Shiraishi Flávio Gobbis, Bazan Rodrigo, Okoshi Katashi, Hueb João Carlos
Faculdade de Medicina de Botucatu (UNESP), Botucatu, SP - Brazil.
Arq Bras Cardiol. 2018 May;110(5):402-410. doi: 10.5935/abc.20180058. Epub 2018 Apr 9.
AIDS as well as atherosclerosis are important public health problems. The longer survival among HIV-infected is associated with increased number of cardiovascular events in this population, and this association is not fully understood.
To identify the frequency of subclinical atherosclerosis in HIV-infected patients compared to control subjects; to analyze associations between atherosclerosis and clinical and laboratory variables, cardiovascular risk factors, and the Framingham coronary heart disease risk score (FCRS).
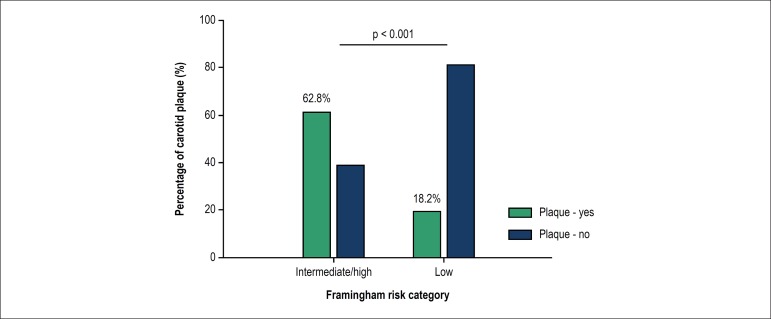
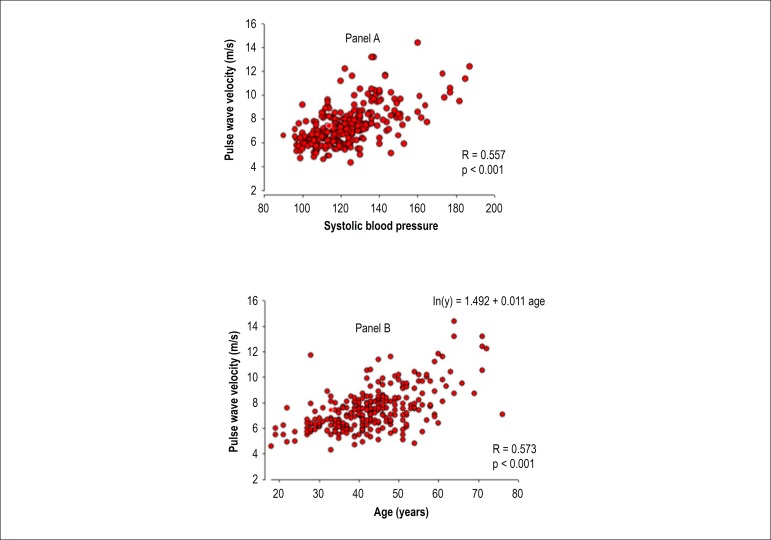
Prospective cross-sectional case-control study assessing the presence of subclinical atherosclerosis in 264 HIV-infected patients and 279 controls. Clinical evaluation included ultrasound examination of the carotid arteries, arterial stiffness by pulse wave velocity (PWV) and augmentation index (AIx), laboratory analysis of peripheral blood, and cardiovascular risk according to FCRS criteria. The significance level adopted in the statistical analysis was p < 0.05.
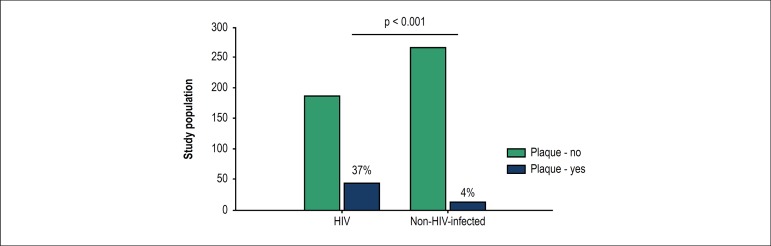
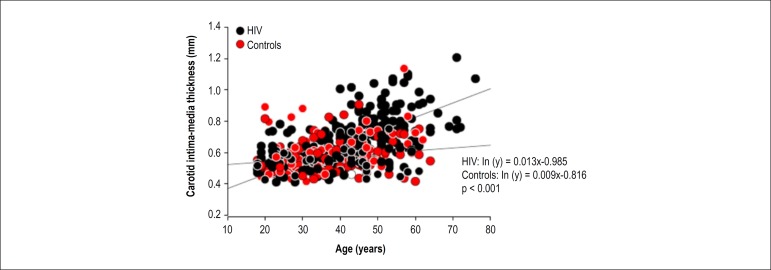
Plaques were found in 37% of the HIV group and 4% of controls (p < 0.001). Furthermore, carotid intima-media thickness was higher in the HIV group than in controls (p < 0.001). Patients with carotid plaque had higher fasting glucose, total cholesterol, low-density lipoprotein cholesterol, and triglycerides than those without plaques. The presence of HIV, adjusted for age, overweight/obesity, and smoking increased by almost fivefold the risk of atherosclerotic carotid plaque (OR: 4.9; 95%CI: 2.5-9.9; p < 0.001). Exposure to protease inhibitors did not influence carotid intima-media thickness, was not associated with carotid plaque frequency, and did not alter the mechanical characteristics of the arterial system (PWV and AIx).
HIV-infected patients are at increased risk of atherosclerosis in association with classical cardiovascular risk factors. Treatment with protease inhibitors does not promote functional changes in the arteries, and shows no association with increased frequency of atherosclerotic plaques in carotid arteries. The FCRS may be inappropriate for this population.
艾滋病和动脉粥样硬化都是重要的公共卫生问题。HIV感染者存活时间延长与该人群心血管事件数量增加有关,而这种关联尚未完全明确。
确定HIV感染者与对照者相比亚临床动脉粥样硬化的发生率;分析动脉粥样硬化与临床和实验室变量、心血管危险因素以及弗雷明汉姆冠心病风险评分(FCRS)之间的关联。
前瞻性横断面病例对照研究,评估264例HIV感染者和279例对照者中亚临床动脉粥样硬化的存在情况。临床评估包括颈动脉超声检查、通过脉搏波速度(PWV)和增强指数(AIx)评估动脉僵硬度、外周血实验室分析以及根据FCRS标准评估心血管风险。统计分析采用的显著性水平为p < 0.05。
HIV组37%的患者发现有斑块,而对照组为4%(p < 0.001)。此外,HIV组的颈动脉内膜中层厚度高于对照组(p < 0.001)。有颈动脉斑块的患者空腹血糖、总胆固醇、低密度脂蛋白胆固醇和甘油三酯水平高于无斑块患者。在调整年龄、超重/肥胖和吸烟因素后,HIV感染使动脉粥样硬化性颈动脉斑块的风险增加近五倍(比值比:4.9;95%置信区间:2.5 - 9.9;p < 0.001)。接触蛋白酶抑制剂不影响颈动脉内膜中层厚度,与颈动脉斑块发生率无关,也未改变动脉系统的力学特性(PWV和AIx)。
HIV感染者发生动脉粥样硬化的风险增加,且与经典心血管危险因素相关。蛋白酶抑制剂治疗不会促进动脉功能改变,也与颈动脉粥样硬化斑块发生率增加无关。FCRS可能不适用于该人群。