Schmitz Roland, Wright George W, Huang Da Wei, Johnson Calvin A, Phelan James D, Wang James Q, Roulland Sandrine, Kasbekar Monica, Young Ryan M, Shaffer Arthur L, Hodson Daniel J, Xiao Wenming, Yu Xin, Yang Yandan, Zhao Hong, Xu Weihong, Liu Xuelu, Zhou Bin, Du Wei, Chan Wing C, Jaffe Elaine S, Gascoyne Randy D, Connors Joseph M, Campo Elias, Lopez-Guillermo Armando, Rosenwald Andreas, Ott German, Delabie Jan, Rimsza Lisa M, Tay Kuang Wei Kevin, Zelenetz Andrew D, Leonard John P, Bartlett Nancy L, Tran Bao, Shetty Jyoti, Zhao Yongmei, Soppet Dan R, Pittaluga Stefania, Wilson Wyndham H, Staudt Louis M
From the Lymphoid Malignancies Branch (R.S., D.W.H., J.D.P., J.Q.W., S.R., M.K., R.M.Y., A.L.S., D.J.H., W. Xiao, X.Y., Y.Y., H.Z., W. Xu, W.H.W., L.M.S.), the Biometric Research Program, Division of Cancer Diagnosis and Treatment (G.W.W.), and the Laboratory of Pathology, Center for Cancer Research (E.S.J., S.P.), National Cancer Institute, and the Office of Intramural Research, Center for Information Technology (C.A.J., X.L., B.Z., W.D.), National Institutes of Health, Bethesda, and the Cancer Research Technology Program, Leidos Biomedical Research, Frederick National Laboratory for Cancer Research, Frederick (B.T., J.S., Y.Z., D.R.S.) - all in Maryland; the Department of Pathology, City of Hope National Medical Center, Duarte, CA (W.C.C.); the BC Cancer Agency, Vancouver, BC (R.D.G., J.M.C.), and the University Health Network, Laboratory Medicine Program, Toronto General Hospital and University of Toronto, Toronto (J.D.) - both in Canada; the Hospital Clinic of Barcelona, University of Barcelona, Institute for Biomedical Research August Pi I Sunyer, Barcelona (E.C., A.L.-G.); the Institute of Pathology, University of Würzburg, and Comprehensive Cancer Center Mainfranken, Würzburg (A.R.), and the Department of Clinical Pathology, Robert-Bosch-Krankenhaus, and Dr. Margarete Fischer-Bosch Institute for Clinical Pharmacology, Stuttgart (G.O.) - all in Germany; the Department of Laboratory Medicine and Pathology, Mayo Clinic, Scottsdale, AZ (L.M.R.); the National Cancer Centre of Singapore, Singapore (K.T.K.W.); Memorial Sloan Kettering Cancer Center (A.D.Z.) and Weill Cornell Medicine (J.P.L.) - both in New York; the Department of Medicine, Washington University School of Medicine, St. Louis (N.L.B.); and the Alliance for Clinical Trials in Oncology, Chicago (A.D.Z., J.P.L., N.L.B.).
N Engl J Med. 2018 Apr 12;378(15):1396-1407. doi: 10.1056/NEJMoa1801445.
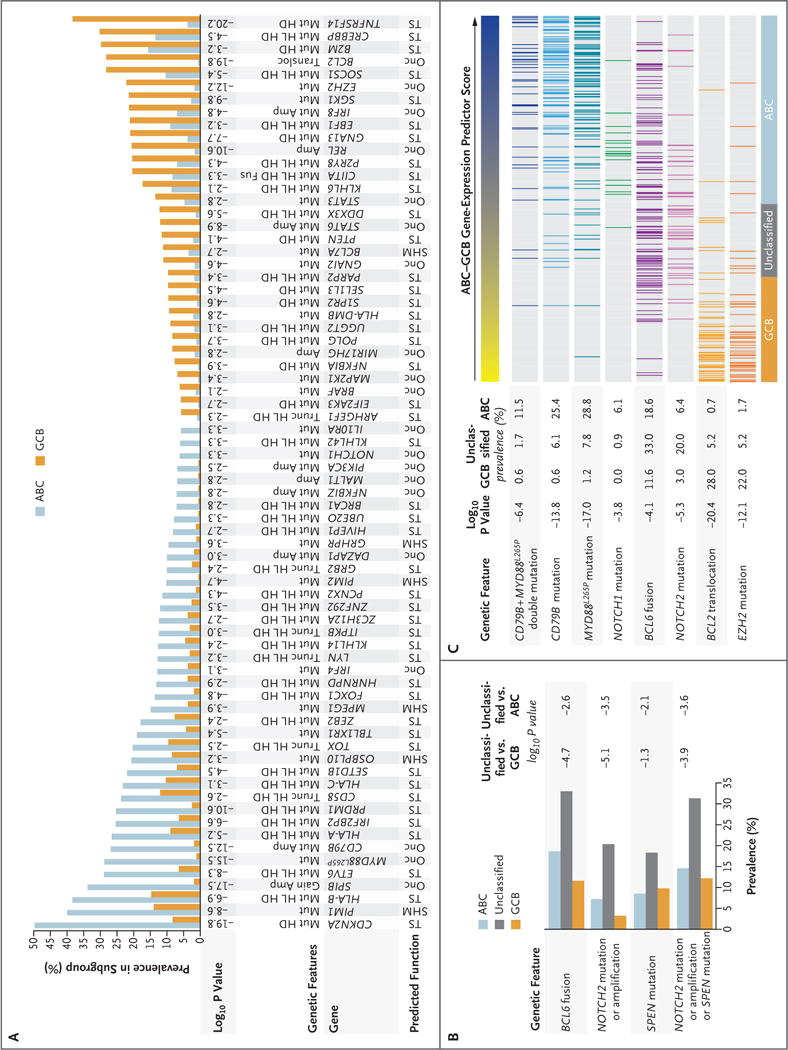
Diffuse large B-cell lymphomas (DLBCLs) are phenotypically and genetically heterogeneous. Gene-expression profiling has identified subgroups of DLBCL (activated B-cell-like [ABC], germinal-center B-cell-like [GCB], and unclassified) according to cell of origin that are associated with a differential response to chemotherapy and targeted agents. We sought to extend these findings by identifying genetic subtypes of DLBCL based on shared genomic abnormalities and to uncover therapeutic vulnerabilities based on tumor genetics.
We studied 574 DLBCL biopsy samples using exome and transcriptome sequencing, array-based DNA copy-number analysis, and targeted amplicon resequencing of 372 genes to identify genes with recurrent aberrations. We developed and implemented an algorithm to discover genetic subtypes based on the co-occurrence of genetic alterations.
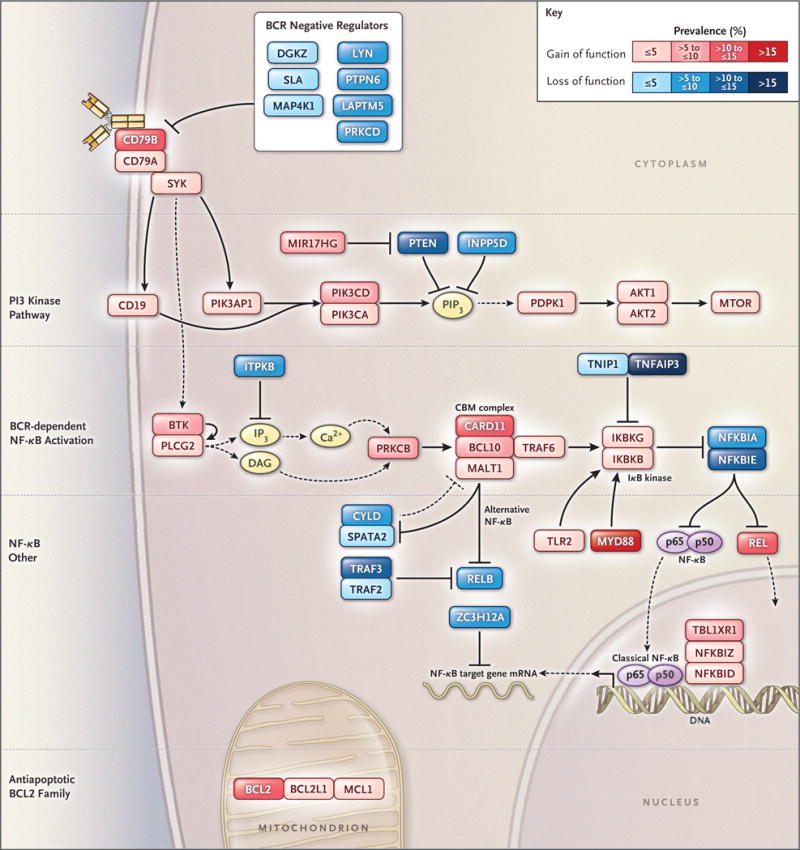
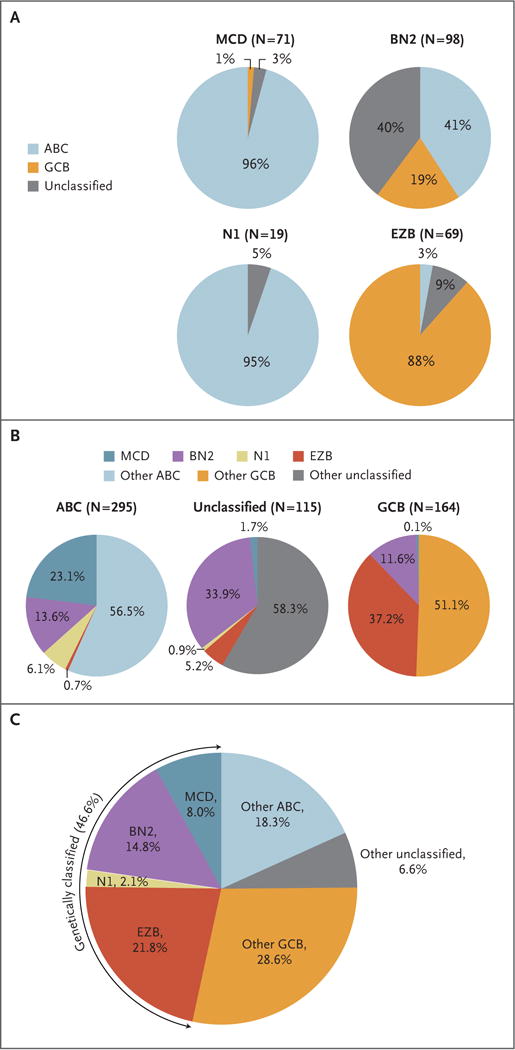
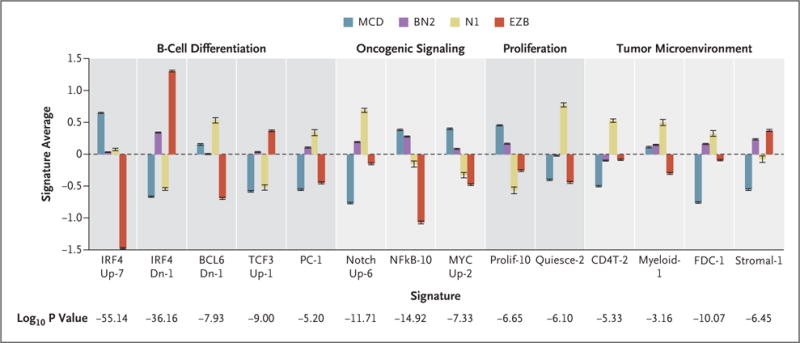
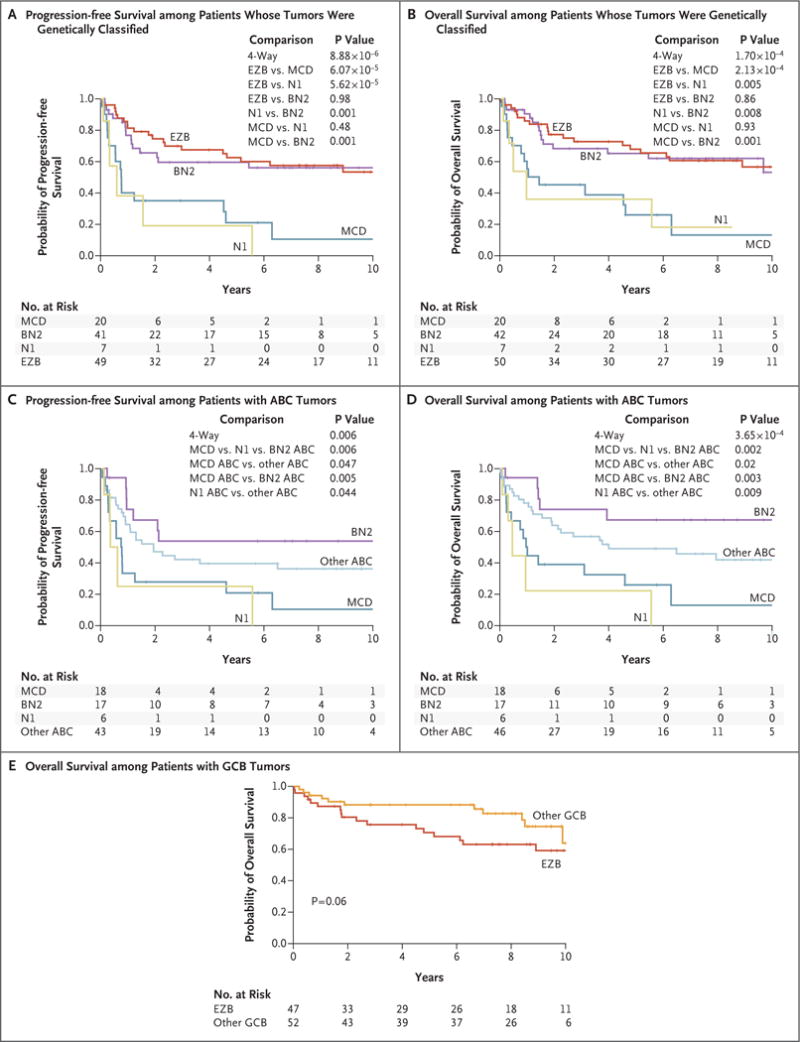
We identified four prominent genetic subtypes in DLBCL, termed MCD (based on the co-occurrence of MYD88 and CD79B mutations), BN2 (based on BCL6 fusions and NOTCH2 mutations), N1 (based on NOTCH1 mutations), and EZB (based on EZH2 mutations and BCL2 translocations). Genetic aberrations in multiple genes distinguished each genetic subtype from other DLBCLs. These subtypes differed phenotypically, as judged by differences in gene-expression signatures and responses to immunochemotherapy, with favorable survival in the BN2 and EZB subtypes and inferior outcomes in the MCD and N1 subtypes. Analysis of genetic pathways suggested that MCD and BN2 DLBCLs rely on "chronic active" B-cell receptor signaling that is amenable to therapeutic inhibition.
We uncovered genetic subtypes of DLBCL with distinct genotypic, epigenetic, and clinical characteristics, providing a potential nosology for precision-medicine strategies in DLBCL. (Funded by the Intramural Research Program of the National Institutes of Health and others.).
弥漫性大B细胞淋巴瘤(DLBCL)在表型和基因上具有异质性。基因表达谱分析已根据起源细胞鉴定出DLBCL的亚组(活化B细胞样[ABC]、生发中心B细胞样[GCB]和未分类),这些亚组与对化疗和靶向药物的不同反应相关。我们试图通过基于共享基因组异常鉴定DLBCL的基因亚型,并基于肿瘤遗传学揭示治疗弱点来扩展这些发现。
我们使用外显子组和转录组测序、基于阵列的DNA拷贝数分析以及对372个基因的靶向扩增子重测序,研究了574份DLBCL活检样本,以鉴定具有复发性畸变的基因。我们开发并实施了一种算法,以基于基因改变的共现来发现基因亚型。
我们在DLBCL中鉴定出四种主要的基因亚型,分别称为MCD(基于MYD88和CD79B突变的共现)、BN2(基于BCL6融合和NOTCH2突变)、N1(基于NOTCH1突变)和EZB(基于EZH2突变和BCL2易位)。多个基因中的基因畸变将每个基因亚型与其他DLBCL区分开来。这些亚型在表型上有所不同,从基因表达特征和对免疫化疗的反应差异判断,BN2和EZB亚型的生存率良好,而MCD和N1亚型的预后较差。对遗传途径的分析表明,MCD和BN2 DLBCL依赖于可通过治疗性抑制的“慢性活跃”B细胞受体信号传导。
我们发现了具有不同基因型、表观遗传和临床特征的DLBCL基因亚型,为DLBCL的精准医学策略提供了潜在的疾病分类学。(由美国国立卫生研究院等的内部研究项目资助。)