Fritz Bradley A, Chen Yixin, Murray-Torres Teresa M, Gregory Stephen, Ben Abdallah Arbi, Kronzer Alex, McKinnon Sherry Lynn, Budelier Thaddeus, Helsten Daniel L, Wildes Troy S, Sharma Anshuman, Avidan Michael Simon
Department of Anesthesiology, Washington University in St Louis, St Louis, Missouri, USA.
Department of Computer Science and Engineering, Washington University in St Louis, St Louis, Missouri, USA.
BMJ Open. 2018 Apr 10;8(4):e020124. doi: 10.1136/bmjopen-2017-020124.
Mortality and morbidity following surgery are pressing public health concerns in the USA. Traditional prediction models for postoperative adverse outcomes demonstrate good discrimination at the population level, but the ability to forecast an individual patient's trajectory in real time remains poor. We propose to apply machine learning techniques to perioperative time-series data to develop algorithms for predicting adverse perioperative outcomes.
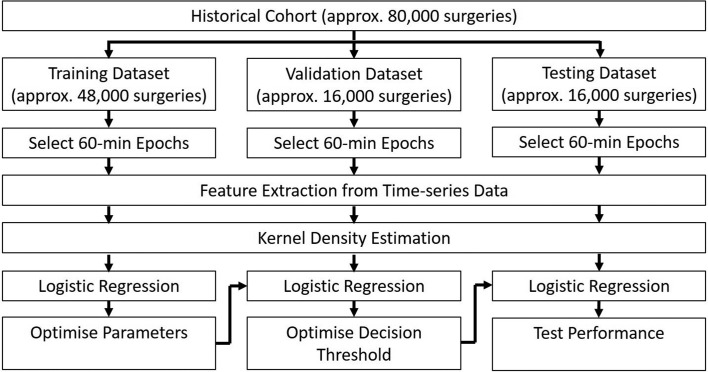
This study will include all adult patients who had surgery at our tertiary care hospital over a 4-year period. Patient history, laboratory values, minute-by-minute intraoperative vital signs and medications administered will be extracted from the electronic medical record. Outcomes will include in-hospital mortality, postoperative acute kidney injury and postoperative respiratory failure. Forecasting algorithms for each of these outcomes will be constructed using density-based logistic regression after employing a Nadaraya-Watson kernel density estimator. Time-series variables will be analysed using first and second-order feature extraction, shapelet methods and convolutional neural networks. The algorithms will be validated through measurement of precision and recall.
This study has been approved by the Human Research Protection Office at Washington University in St Louis. The successful development of these forecasting algorithms will allow perioperative healthcare clinicians to predict more accurately an individual patient's risk for specific adverse perioperative outcomes in real time. Knowledge of a patient's dynamic risk profile may allow clinicians to make targeted changes in the care plan that will alter the patient's outcome trajectory. This hypothesis will be tested in a future randomised controlled trial.
在美国,手术相关的死亡率和发病率是紧迫的公共卫生问题。传统的术后不良结局预测模型在人群层面显示出良好的区分度,但实时预测个体患者病程的能力仍然较差。我们建议将机器学习技术应用于围手术期时间序列数据,以开发预测围手术期不良结局的算法。
本研究将纳入在我们三级医疗中心4年内接受手术的所有成年患者。患者病史、实验室检查值、术中逐分钟生命体征及所用药物将从电子病历中提取。结局指标将包括院内死亡率、术后急性肾损伤和术后呼吸衰竭。在使用Nadaraya-Watson核密度估计器后,将采用基于密度的逻辑回归构建这些结局指标各自的预测算法。时间序列变量将使用一阶和二阶特征提取、形状let方法和卷积神经网络进行分析。这些算法将通过测量精度和召回率进行验证。
本研究已获得圣路易斯华盛顿大学人类研究保护办公室的批准。这些预测算法的成功开发将使围手术期医疗保健临床医生能够实时更准确地预测个体患者发生特定围手术期不良结局的风险。了解患者的动态风险概况可能使临床医生对护理计划进行有针对性的调整,从而改变患者的病程轨迹。这一假设将在未来的随机对照试验中进行检验。