Centro de Investigação em Saúde de Manhiça (CISM), Maputo, Mozambique.
ISGlobal, Barcelona Institute for Global Health, Hospital Clínic - Universitat de Barcelona, Barcelona, Spain.
J Int AIDS Soc. 2018 Apr;21(4):e25095. doi: 10.1002/jia2.25095.
Awareness of HIV-infection goes beyond diagnosis, and encompasses understanding, acceptance, disclosure and initiation of the HIV-care. We aimed to characterize the HIV-positive population that underwent repeat HIV-testing without disclosing their serostatus and the impact on estimates of the first UNAIDS 90 target.
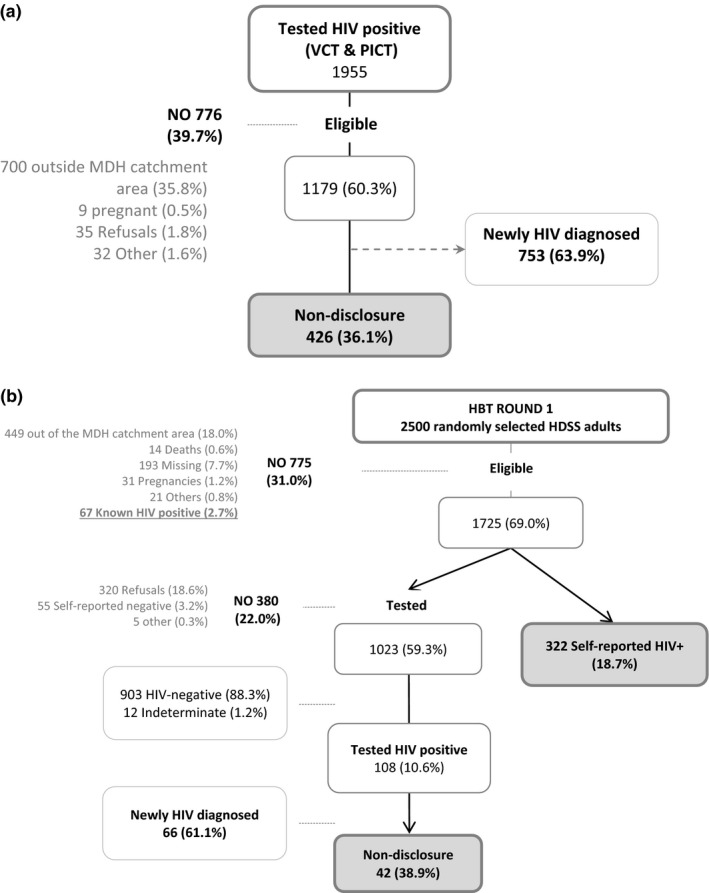
This analysis was nested in a prospective cohort established in southern Mozambique which conducted three HIV-testing modalities: voluntary counselling and testing (VCT), provider-initiated counselling and testing (PICT) and home-based testing (HBT). Participants were given the opportunity to self-report their status to lay counsellors and HIV-positive diagnoses were verified for previous enrolment in care. This study included 1955 individuals diagnosed with HIV through VCT/PICT and 11,746 participants of a HBT campaign. Those who did not report their serostatus prior to testing, and were found to have a previous HIV-diagnosis, were defined as non-disclosures. Venue-stratified descriptive analyses were performed and factors associated with non-disclosure were estimated through log-binomial regression.
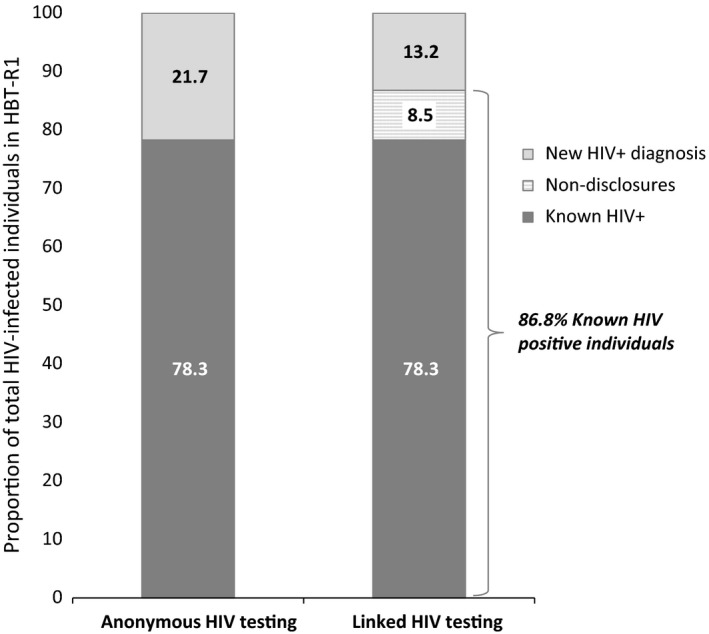
In the first round of 2500 adults randomized for HBT, 1725 were eligible for testing and 18.7% self-reported their HIV-positivity. Of those tested with a positive result, 38.9% were found to be non-disclosures. Similar prevalence of non-disclosures was found in clinical-testing modalities, 29.4% (95% CI 26.7 to 32.3) for PICT strategy and 13.0% (95% CI 10.9 to 15.3) for VCT. Prior history of missed visits (adjusted prevalence ratio (APR) 4.2, 95% CI 2.6 to 6.8), younger age (APR 2.5, 95% CI 1.4 to 4.4) and no prior history of treatment ((APR) 1.4, 95% CI 1.0 to 2.1) were significantly associated with non-disclosure as compared to patients who self-reported. When considering non-disclosures as people living with HIV (PLWHIV) aware of their HIV-status, the proportion of PLWHIV aware increased from 78.3% (95% CI 74.2 to 81.6) to 86.8% (95% CI 83.4 to 89.6).
More than one-third of individuals testing HIV-positive did not disclose their previous positive HIV-diagnosis to counsellors. This proportion varied according to testing modality and age. In the absence of an efficient and non-anonymous tracking system for HIV-testers, repeat testing of non-disclosures leads to wasted resources and may distort programmatic indicators. Developing interventions that ensure appropriate psychosocial support are needed to encourage this population to disclose their status and optimize scarce resources.
艾滋病病毒感染的意识不仅限于诊断,还包括对艾滋病病毒的了解、接受、披露和艾滋病护理的启动。我们旨在描述那些在未披露其血清阳性状态的情况下接受重复艾滋病病毒检测的艾滋病病毒阳性人群,并评估这对实现联合国艾滋病规划署 90 目标的第一项的影响。
这项分析是嵌套在莫桑比克南部建立的一个前瞻性队列研究中,该研究采用了三种艾滋病病毒检测方式:自愿咨询和检测(VCT)、医务人员发起的咨询和检测(PICT)和家庭检测(HBT)。参与者有机会向初级咨询员报告自己的状况,而以前登记的艾滋病病毒感染者则被确认为阳性。这项研究包括通过 VCT/PICT 诊断的 1955 名艾滋病病毒感染者和 11746 名参加 HBT 运动的参与者。那些在检测前未报告其血清阳性状态且以前被诊断为艾滋病病毒感染者的人被定义为未披露者。对按地点分层的描述性分析进行了分析,并通过对数二项式回归估计了与未披露相关的因素。
在 HBT 中随机分配的 2500 名成年人的第一轮中,有 1725 人符合检测条件,其中 18.7%自我报告了其艾滋病病毒阳性。在检测呈阳性的人中,有 38.9%的人未披露。在临床检测方式中也发现了类似的未披露比例,医务人员发起的咨询和检测策略为 29.4%(95%置信区间 26.7 至 32.3),自愿咨询和检测为 13.0%(95%置信区间 10.9 至 15.3)。与自我报告的患者相比,先前错过就诊的经历(调整后的患病率比(APR)4.2,95%置信区间 2.6 至 6.8)、年龄较小(APR 2.5,95%置信区间 1.4 至 4.4)和无既往治疗史(APR 1.4,95%置信区间 1.0 至 2.1)与未披露显著相关。当将未披露者视为知晓其艾滋病毒状况的艾滋病毒感染者(PLHIV)时,知晓其艾滋病毒状况的 PLHIV 比例从 78.3%(95%置信区间 74.2 至 81.6)增加到 86.8%(95%置信区间 83.4 至 89.6)。
超过三分之一的艾滋病病毒检测呈阳性的人未向咨询员披露其以前的艾滋病病毒阳性诊断。这一比例因检测方式和年龄而异。在缺乏高效且非匿名的艾滋病病毒检测者追踪系统的情况下,对未披露者的重复检测会浪费资源,并可能扭曲项目指标。需要制定确保适当社会心理支持的干预措施,以鼓励这部分人群披露其状况并优化有限的资源。