Department of Neurosurgery, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
Clinical Neuroscience Center, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
BMC Neurol. 2021 Jul 22;21(1):285. doi: 10.1186/s12883-021-02322-5.
Brain biopsies are crucial diagnostic interventions, providing valuable information for treatment and prognosis, but largely depend on a high accuracy and precision. We hypothesized that through the combination of neuronavigation-based frameless stereotaxy and MRI-guided trajectory planning with intraoperative CT examination using a mobile unit, one can achieve a seamlessly integrated approach yielding optimal target accuracy.
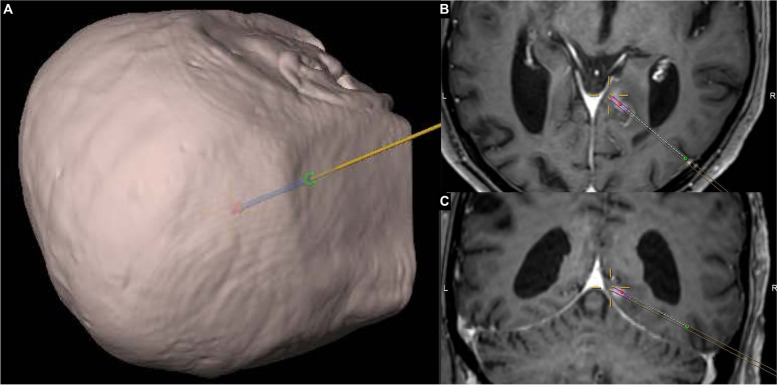
We analyzed a total of 7 stereotactic biopsy trajectories for a variety of deep-seated locations and different patient positions. After rigid head fixation, an intraoperative pre-procedural scan using a mobile CT unit was performed for automatic image fusion with the planning MRI images and a peri-procedural scan with the biopsy cannula in situ for verification of the definite target position. We then evaluated the radial trajectory error.
Intraoperative scanning, surgery, computerized merging of MRI and CT images as well as trajectory planning were feasible without difficulties and safe in all cases. We achieved a radial trajectory deviation of 0.97 ± 0.39 mm at a trajectory length of 60 ± 12.3 mm (mean ± standard deviation). Repositioning of the biopsy cannula due to inaccurate targeting was not required.
Intraoperative verification using a mobile CT unit in combination with frameless neuronavigation-guided stereotaxy and pre-operative MRI-based trajectory planning was feasible, safe and highly accurate. The setting enabled single-millimeter accuracy for deep-seated brain lesions and direct detection of intraoperative complications, did not depend on a dedicated operating room and was seamlessly integrated into common stereotactic procedures.
脑活检是至关重要的诊断干预措施,可为治疗和预后提供有价值的信息,但在很大程度上依赖于高度的准确性和精密度。我们假设,通过结合基于神经导航的无框架立体定向和 MRI 引导的轨迹规划,并在术中使用移动单元进行 CT 检查,可以实现一种无缝集成的方法,从而获得最佳的目标准确性。
我们分析了总共 7 例用于各种深部位置和不同患者体位的立体定向活检轨迹。在刚性头部固定后,使用移动 CT 单元进行术中预手术扫描,以便与计划 MRI 图像自动进行图像融合,并对在位的活检套管进行术中扫描,以验证明确的目标位置。然后,我们评估了径向轨迹误差。
在所有情况下,术中扫描、手术、MRI 和 CT 图像的计算机化合并以及轨迹规划都是可行的,没有困难且安全。我们在 60±12.3mm 的轨迹长度上实现了 0.97±0.39mm 的径向轨迹偏差(平均值±标准差)。由于定位不准确而需要重新定位活检套管的情况并不需要。
使用移动 CT 单元结合无框架神经导航引导立体定向和术前基于 MRI 的轨迹规划进行术中验证是可行的、安全的和高度准确的。该设置实现了深部脑病变的毫米级精度和术中并发症的直接检测,不依赖于专用手术室,并与常规立体定向手术无缝集成。