Department of Pharmacy Practice, University of Connecticut School of Pharmacy, Storrs, CT.
Evidence-Based Practice Center, Hartford Hospital, Hartford, CT.
J Am Heart Assoc. 2018 Apr 13;7(8):e008643. doi: 10.1161/JAHA.118.008643.
Frailty predicts poorer outcomes and decreased anticoagulation use in patients with nonvalvular atrial fibrillation. We sought to assess the effectiveness and safety of apixaban, dabigatran and rivaroxaban versus warfarin in frail nonvalvular atrial fibrillation patients.
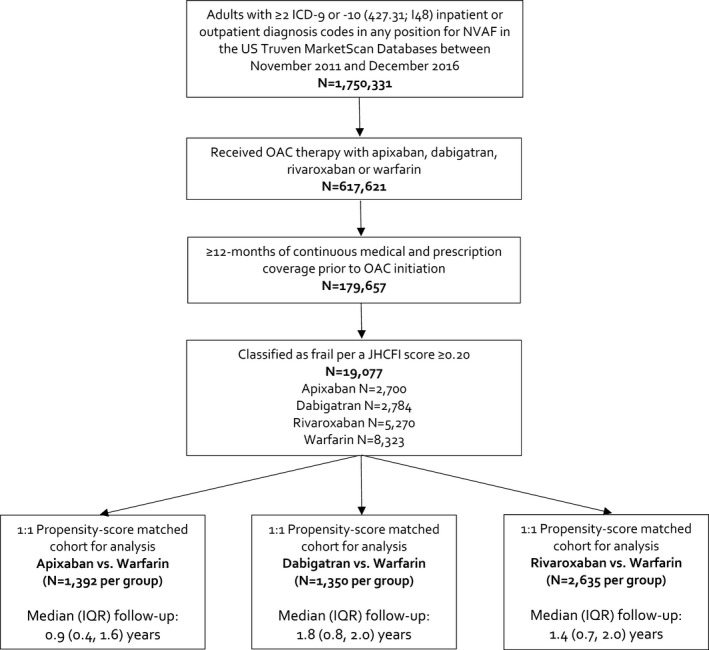
Using US MarketScan claims data from November 2011 to December 2016, we identified frail oral anticoagulant-naïve nonvalvular atrial fibrillation patients with ≥12 months of continuous insurance coverage before oral anticoagulant initiation. Frailty status was determined using the Johns Hopkins Claims-based Frailty Indicator score (≥0.20 indicating frailty). Users of apixaban, dabigatran, or rivaroxaban were separately 1:1 matched to warfarin users via propensity-scores, with residual absolute standardized differences <0.1 being achieved for all covariates after matching. Patients were followed for up to 2 years or until an event, insurance disenrollment or end of follow-up. Rates of stroke or systemic embolism and major bleeding were compared using Cox regression and reported as hazard ratios (HRs) and 95% confidence intervals (CIs). In total, 2700, 2784, and 5270 patients were included in the apixaban, dabigatran, and rivaroxaban 1:1 matched analyses to warfarin. At 2 years, neither apixaban nor dabigatran were associated with differences in the hazard of stroke or systemic embolism (HR=0.78; 95% CI=0.46-1.35 and HR=0.94; 0.60-1.45) or major bleeding (HR=0.72; 95% CI=0.49-1.06 and HR=0.87; 95% CI=0.63-1.19) versus warfarin. Rivaroxaban was associated with reduced stroke or systemic embolism at 2 years (HR=0.68; 95% CI=0.49-0.95) without significantly altering major bleeding risk (HR=1.07; 95% CI=0.81-1.32).
Our study found rivaroxaban but not apixaban or dabigatran to be associated with reduced SSE versus warfarin in frail nonvalvular atrial fibrillation patients. No direct-acting oral anticoagulants demonstrated a significant difference in major bleeding versus warfarin.
衰弱预测非瓣膜性心房颤动患者的预后较差和抗凝药物使用率降低。我们旨在评估阿哌沙班、达比加群和利伐沙班与华法林相比在衰弱的非瓣膜性心房颤动患者中的疗效和安全性。
使用 2011 年 11 月至 2016 年 12 月期间美国 MarketScan 理赔数据,我们确定了衰弱的口服抗凝剂初治非瓣膜性心房颤动患者,这些患者在开始口服抗凝治疗前有≥12 个月的连续保险覆盖。使用约翰霍普金斯基于索赔的衰弱指标评分(≥0.20 表示衰弱)来确定衰弱状态。阿哌沙班、达比加群或利伐沙班的使用者分别通过倾向评分与华法林使用者 1:1 匹配,匹配后所有协变量的残余绝对标准化差异均<0.1。患者随访时间最长为 2 年或直至发生事件、保险退保或随访结束。使用 Cox 回归比较卒中或全身性栓塞和大出血的发生率,并以风险比(HR)和 95%置信区间(CI)报告。在阿哌沙班、达比加群和利伐沙班 1:1 匹配分析中,分别有 2700、2784 和 5270 例患者纳入华法林组。2 年时,阿哌沙班和达比加群与华法林相比,卒中或全身性栓塞(HR=0.78;95%CI=0.46-1.35 和 HR=0.94;0.60-1.45)或大出血(HR=0.72;95%CI=0.49-1.06 和 HR=0.87;95%CI=0.63-1.19)的风险无差异。利伐沙班与 2 年时的卒中或全身性栓塞降低相关(HR=0.68;95%CI=0.49-0.95),但不显著改变大出血风险(HR=1.07;95%CI=0.81-1.32)。
我们的研究发现,与华法林相比,利伐沙班而非阿哌沙班或达比加群与衰弱的非瓣膜性心房颤动患者的 SSE 降低相关。与华法林相比,没有一种直接作用的口服抗凝剂在大出血方面显示出显著差异。