Aboelsoud Mohammed, Siddique Osama, Morales Alexander, Seol Young, Al-Qadi Mazen
Department of Medicine, Memorial Hospital of Rhode Island, Alpert Medical School of Brown University, Providence, USA.
Division of Pulmonary, Critical Care and Sleep Medicine, Providence, USA.
Prz Gastroenterol. 2018;13(1):16-21. doi: 10.5114/pg.2018.74557. Epub 2018 Mar 26.
Acute cholangitis (AC) is a clinical condition that requires prompt medical management with IV fluids, antibiotics, and biliary drainage (BD). The optimal timing for BD remains unclear.
To investigate the effect of biliary drainage timing on clinical outcomes in AC.
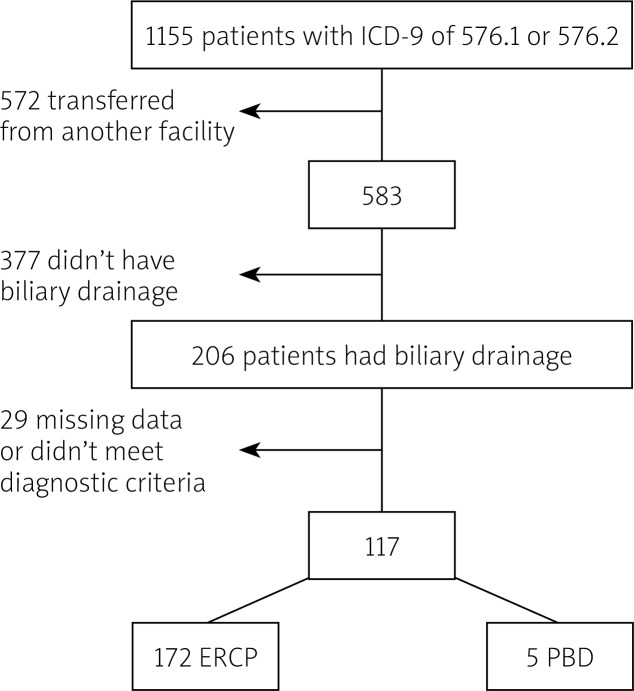
We conducted a retrospective study of patients with AC admitted to the ICU using the Multiparameter Intelligent Monitoring in Intensive Care III (MIMIC-III) database. Emergency department to BD time, hospital death, length of stay (LOS), and severity scores were extracted from the database. We investigated the effect of BD timing on mortality rates, persistent organ failure, and LOS.
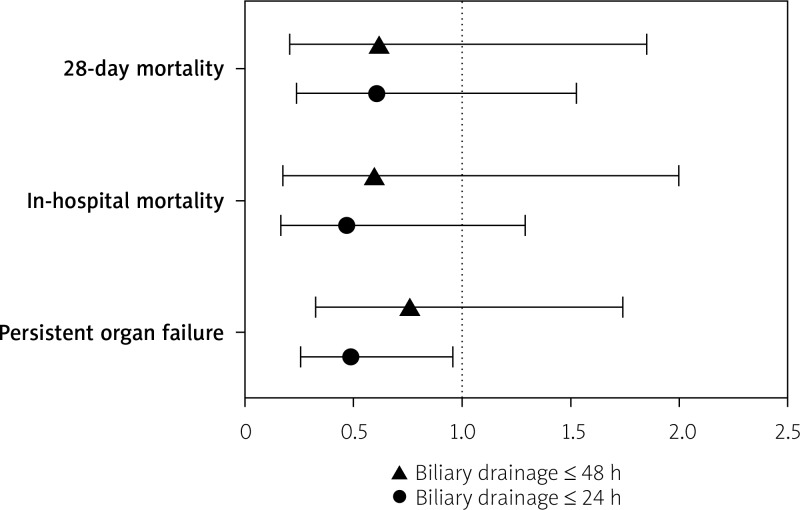
A total of 177 patients were included; 50% were males; median age was 75 years, in-hospital mortality was 9.6%, mean time-to-ERCP was 32 h (range: 0.42-229.6) with 76% meeting the Tokyo Guidelines (TG13) criteria for severe cholangitis, and median Simplified Acute Physiology Score II (SAPS II) was 42 (IQR: 33-51). Using 24 h as a cut-off, patients who underwent BD ≤ 24 h had less persistent organ failure (OR = 0.49; 95% CI: 0.26-0.96, = 0.040), shorter ICU LOS (3.25 vs. 4.95 days, = 0.040), shorter hospital LOS (7.71 vs. 13.57 days, = 0.001), but no difference in either in-hospital mortality (OR = 0.47, 95% CI: 0.17-1.29, = 0.146) or 28-day mortality (OR = 0.61, 95% CI: 0.24-1.53, = 0.297).
In critically-ill patients with acute cholangitis, early biliary drainage ≤ 24 h is associated with less persistent organ failure and shorter length of stay but had no effect on patient survival.
急性胆管炎(AC)是一种临床病症,需要通过静脉输液、使用抗生素及胆道引流(BD)进行及时治疗。BD的最佳时机仍不明确。
探讨胆道引流时机对AC临床结局的影响。
我们使用重症监护多参数智能监测数据库III(MIMIC-III)对入住重症监护病房(ICU)的AC患者进行了一项回顾性研究。从数据库中提取急诊科至BD的时间、医院死亡情况、住院时间(LOS)及严重程度评分。我们研究了BD时机对死亡率、持续性器官衰竭及LOS的影响。
共纳入177例患者;50%为男性;中位年龄为75岁,住院死亡率为9.6%,平均至内镜逆行胰胆管造影(ERCP)时间为32小时(范围:0.42 - 229.6),76%符合东京指南(TG13)严重胆管炎标准,简化急性生理学评分II(SAPS II)中位数为42(四分位间距:33 - 51)。以24小时为界值,在24小时内接受BD的患者持续性器官衰竭较少(比值比[OR]=0.49;95%置信区间[CI]:0.26 - 0.96,P = 0.040),ICU住院时间较短(3.25天对4.95天,P = 0.040),医院住院时间较短(7.71天对13.57天,P = 0.001),但住院死亡率(OR = 0.47,95% CI:0.17 - 1.29,P = 0.146)或28天死亡率(OR = 0.61,95% CI:0.24 - 1.53,P = 0.297)均无差异。
在患有急性胆管炎的重症患者中,早期胆道引流(≤24小时)与较少的持续性器官衰竭及较短的住院时间相关,但对患者生存无影响。