Jansen Diahann T S L, Emery Paul, Smolen Josef S, Westhovens Rene, Le Bars Manuela, Connolly Sean E, Ye June, Toes René E M, Huizinga Tom W J
Department of Rheumatology, Leiden University Medical Center, Leiden, The Netherlands.
Leeds Musculoskeletal Biomedical Research Unit, LTHT Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, UK.
RMD Open. 2018 Mar 30;4(1):e000564. doi: 10.1136/rmdopen-2017-000564. eCollection 2018.
To evaluate the effects of the T-cell costimulation blocker abatacept on anti-citrullinated protein antibodies (ACPA) and rheumatoid factor (RF) in early rheumatoid arthritis (RA), and associations between changes in serological status and clinical response.
Post hoc analysis of the phase III AGREE study in methotrexate (MTX)-naïve patients with early RA and poor prognostic factors. Patients were randomised to abatacept (~10 mg/kg intravenously according to weight range) or placebo, plus MTX over 12 months followed by open-label abatacept plus MTX for 12 months. Autoantibody titres were determined by ELISA at baseline and months 6 and 12 (double-blind phase). Conversion to seronegative status and its association with clinical response were assessed at months 6 and 12.
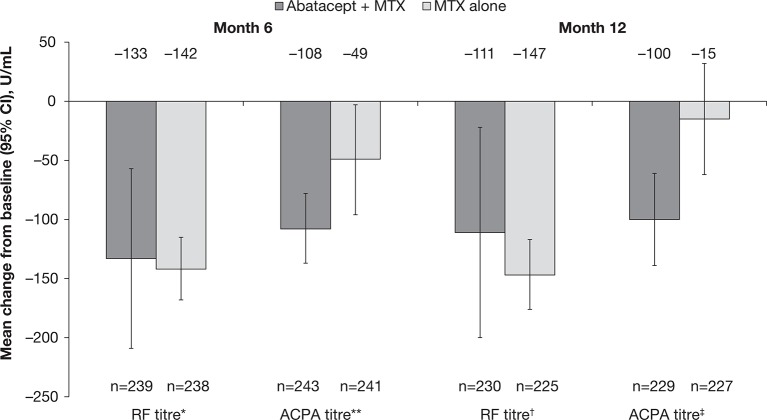
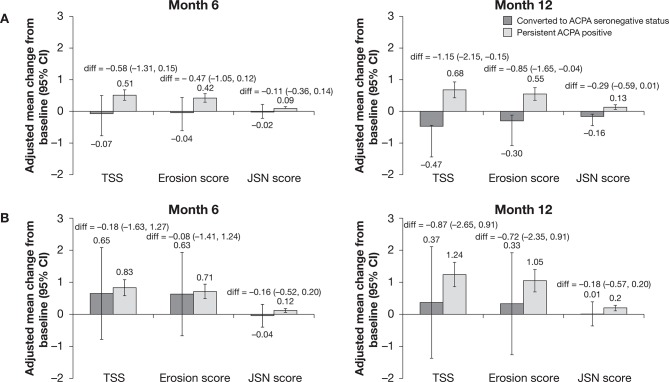
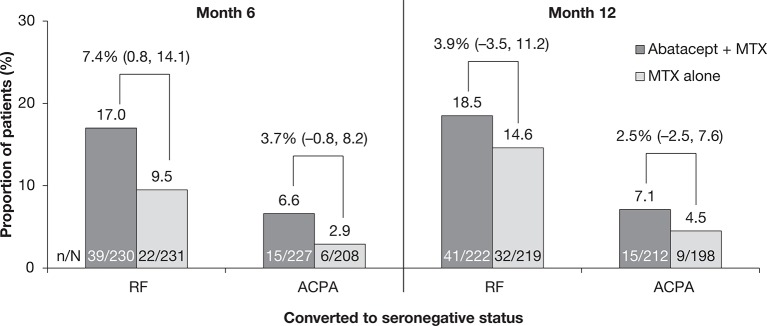
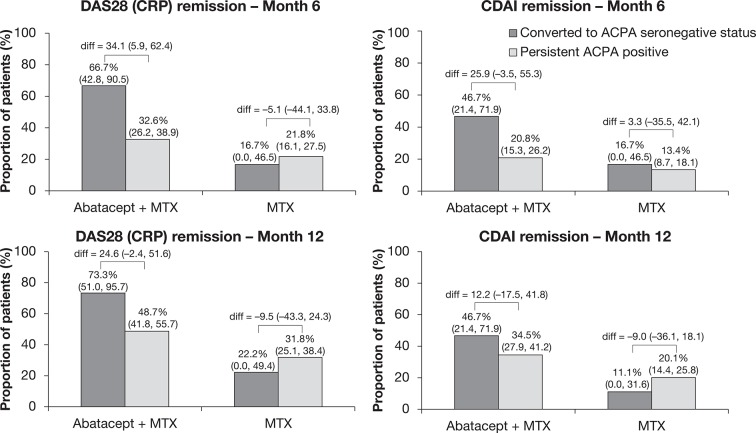
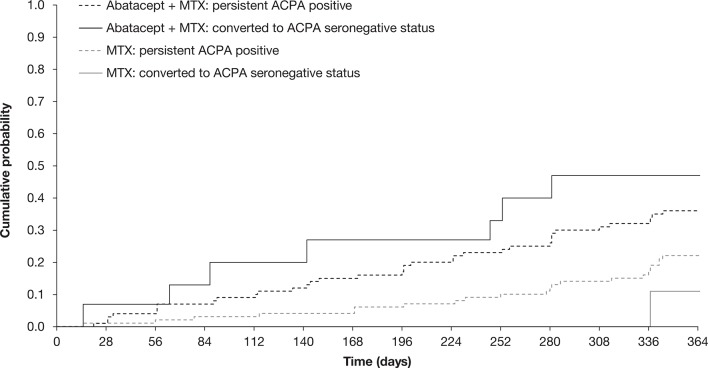
Abatacept plus MTX was associated with a greater decrease in ACPA (but not RF) titres and higher rates of both ACPA and RF conversion to seronegative status versus MTX alone. More patients converting to ACPA seronegative status receiving abatacept plus MTX achieved remission according to Disease Activity Score in 28 joints (C-reactive protein) or Clinical Disease Activity Index than patients who remained ACPA seropositive. Patients who converted to ACPA seronegative status treated with abatacept plus MTX had a greater probability of achieving sustained remission and less radiographic progression than MTX alone or patients who remained ACPA seropositive (either treatment).
Treatment with abatacept plus MTX was more likely to induce conversion to ACPA/RF seronegative status in patients with early, erosive RA. Conversion to ACPA seronegative status was associated with better clinical and radiographic outcomes.
NCT00122382.
评估T细胞共刺激阻滞剂阿巴西普对早期类风湿关节炎(RA)患者抗瓜氨酸化蛋白抗体(ACPA)和类风湿因子(RF)的影响,以及血清学状态变化与临床反应之间的关联。
对一项III期AGREE研究进行事后分析,该研究纳入了未使用甲氨蝶呤(MTX)且具有不良预后因素的早期RA患者。患者被随机分为阿巴西普组(根据体重范围静脉注射约10 mg/kg)或安慰剂组,同时联合MTX治疗12个月,随后开放标签使用阿巴西普联合MTX治疗12个月。在基线、第6个月和第12个月(双盲阶段)通过酶联免疫吸附测定法(ELISA)测定自身抗体滴度。在第6个月和第12个月评估转为血清阴性状态及其与临床反应的关联。
与单独使用MTX相比,阿巴西普联合MTX可使ACPA(而非RF)滴度更大幅度降低,且ACPA和RF转为血清阴性状态的比例更高。根据28个关节疾病活动评分(C反应蛋白)或临床疾病活动指数,转为ACPA血清阴性状态并接受阿巴西普联合MTX治疗的患者比仍为ACPA血清阳性的患者达到缓解的更多。与单独使用MTX或仍为ACPA血清阳性的患者(无论接受何种治疗)相比,接受阿巴西普联合MTX治疗并转为ACPA血清阴性状态的患者实现持续缓解的可能性更大,影像学进展更少。
对于早期、侵蚀性RA患者,阿巴西普联合MTX治疗更有可能诱导转为ACPA/RF血清阴性状态。转为ACPA血清阴性状态与更好的临床和影像学结局相关。
NCT00122382。