Critical Care and Anesthesiology Research Group, Stavanger University Hospital, Stavanger, Norway.
Norwegian Air Ambulance Foundation, Department of Research and Development, Drøbak, Norway.
Crit Care. 2018 Apr 18;22(1):99. doi: 10.1186/s13054-018-2017-x.
The modifiable prehospital system factors, bystander cardiopulmonary resuscitation (CPR), emergency medical services (EMS), response time, and EMS physician attendance, may affect short- and long-term survival for both rural and urban out-of-hospital cardiac arrest (OHCA) patients. We studied how such factors influenced OHCA survival in a mixed urban/rural region with a high survival rate after OHCA.
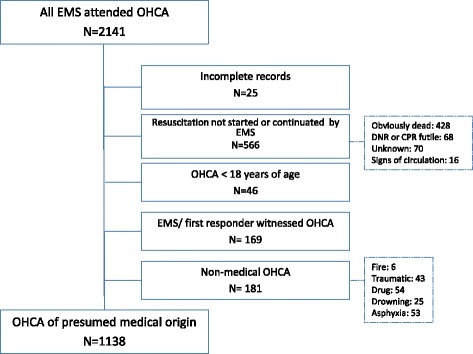
We analyzed the association between modifiable prehospital factors and survival to different stages of care in 1138 medical OHCA patients from an Utstein template-based cardiac arrest registry, using Kaplan-Meier type survival curves, univariable and multivariable logistic regression and mortality hazard plots.
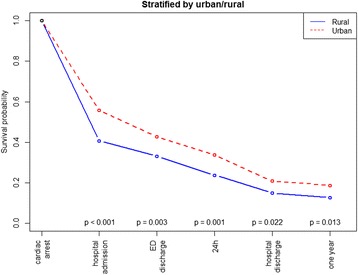
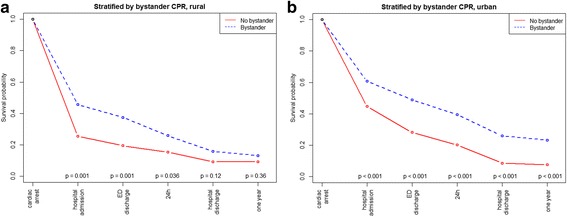
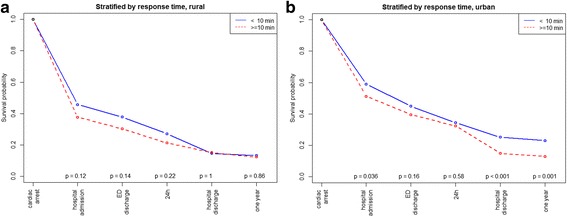
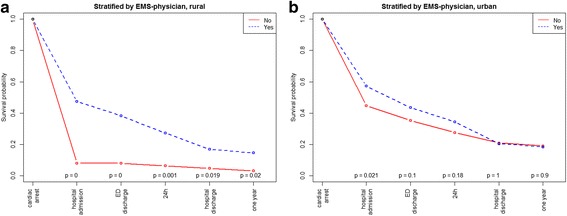
We found a significantly higher probability for survival to hospital admission (OR: 1.84, 95% CI 1.43-2.36, p < 0.001), to hospital discharge (OR: 1.51, 95% CI 1.08-2.11, p = 0.017), and at 1 year (OR: 1.58, 95% CI 1.11-2.26, p = 0.012) in the urban group versus the rural group. In patients receiving bystander CPR before EMS arrival, the odds of survival to hospital discharge increased more than threefold (OR: 3.05, 95% CI 2.00-4.65, p < 0.001). However, bystander CPR was associated with increased patient survival to discharge only in urban areas (survival probability 0.26 with CPR vs. 0.08 without CPR, p < 0.001). EMS response time ≥ 10 min was associated with decreased survival (OR: 0.61, 95% CI 0.45-0.83, p = 0.002), however, only in urban areas (survival probability 0.15 ≥ 10 min vs. 0.25 < 10 min, p < 0.001). In patients with prehospital EMS physician attendance, no significant differences were found in survival to hospital discharge (OR: 1.37, 95% CI 0.87-2.16, p = 0.17). In rural areas, patients with EMS physician attendance had an overall better survival to hospital discharge (survival probability 0.17 with EMS physician vs. 0.05 without EMS physician, p = 0.019). Adjusted for modifiable factors, the survival differences remained.
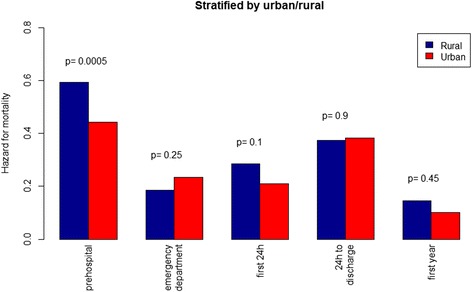
Overall, OHCA survival was higher in urban compared to rural areas, and the effect of bystander CPR, EMS response time and EMS physician attendance on survival differ between urban and rural areas. The effect of modifiable factors on survival was highest in the prehospital stage of care. In patients surviving to hospital admission, there was no significant difference in in-hospital mortality or in 1 year mortality between OHCA in rural versus urban areas.
可改变的院前系统因素,包括旁观者心肺复苏(CPR)、紧急医疗服务(EMS)、反应时间和 EMS 医生到场,可能会影响农村和城市院外心脏骤停(OHCA)患者的短期和长期生存。我们研究了在 OHCA 后生存率较高的混合城乡地区,这些因素如何影响 OHCA 患者的生存。
我们使用 Kaplan-Meier 类型生存曲线、单变量和多变量逻辑回归以及死亡率风险图,分析了来自基于 Utstein 模板的心脏骤停登记处的 1138 例医学 OHCA 患者的可改变院前因素与不同阶段治疗的生存之间的关联。
我们发现,与农村组相比,城市组患者入院(OR:1.84,95%CI 1.43-2.36,p<0.001)、出院(OR:1.51,95%CI 1.08-2.11,p=0.017)和 1 年(OR:1.58,95%CI 1.11-2.26,p=0.012)的存活概率更高。在 EMS 到达前接受旁观者 CPR 的患者中,出院存活的几率增加了三倍以上(OR:3.05,95%CI 2.00-4.65,p<0.001)。然而,旁观者 CPR 仅在城市地区与患者出院后存活增加相关(CPR 组的存活概率为 0.26,无 CPR 组为 0.08,p<0.001)。EMS 反应时间≥10 分钟与存活下降相关(OR:0.61,95%CI 0.45-0.83,p=0.002),但仅在城市地区(反应时间≥10 分钟组的存活概率为 0.15,反应时间<10 分钟组为 0.25,p<0.001)。在有院前 EMS 医生出勤的患者中,出院时的存活无显著差异(OR:1.37,95%CI 0.87-2.16,p=0.17)。在农村地区,有 EMS 医生出勤的患者总体上出院后存活更好(有 EMS 医生的存活概率为 0.17,无 EMS 医生的存活概率为 0.05,p=0.019)。调整可改变因素后,存活差异仍然存在。
总体而言,城市地区 OHCA 患者的生存率高于农村地区,旁观者 CPR、EMS 反应时间和 EMS 医生出勤对生存率的影响在城乡地区不同。可改变因素对生存的影响在院前治疗阶段最高。在入院后存活的患者中,农村地区与城市地区 OHCA 患者的院内死亡率或 1 年死亡率无显著差异。