Division of Gastroenterology & Hepatology, Department of Medicine.
Department of Preventive Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL.
Hepatology. 2018 Oct;68(4):1633-1641. doi: 10.1002/hep.30048. Epub 2018 Sep 22.
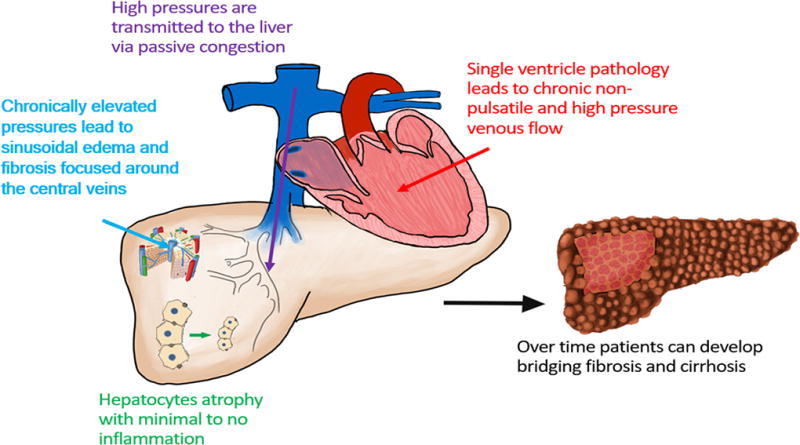
Congestive hepatopathy (CH) arises from chronically elevated right-sided heart pressures transmitted to the liver by passive venous congestion. Over time, CH can lead to hepatic bridging fibrosis, decompensated cirrhosis, and hepatocellular carcinoma. Currently, there are no evidence-based guidelines to direct appropriate screening or management of patients with CH, partly because of the inability of current clinical tools (serum tests, imaging studies, liver stiffness measurements, and liver biopsy) to accurately estimate hepatic fibrosis or the risk for hepatic decompensation. The Model for End-Stage Liver Disease excluding international normalized ratio (MELD-XI) score is the only validated serum-based test to predict clinical outcomes in CH. Noninvasive liver stiffness measurements are proving to be of minimal utility as all patients with CH have elevated values that currently cannot differentiate between congestion and fibrosis. In addition, fibrosis staging by liver biopsy is difficult to standardize because of heterogeneous collagen deposition in CH. Moreover, liver biopsy results have little predictive value for post-heart transplant hepatic outcomes in patients with CH. Evaluating liver nodules and masses is also complicated in CH as the finding of delayed venous washout in nodules is not specific for hepatocellular carcinoma in the background of a congested liver, and these lesions may require biopsy to confirm the diagnosis. The lack of effective clinical tools for predicting liver fibrosis and liver function suggests the need for the development of novel biomarkers in patients with CH to assist in the management of this complicated disease. (Hepatology 2018; 00:000-000).
充血性肝病原发性于右侧心腔压力持续升高,升高的压力通过被动性静脉淤血传递到肝脏。随着时间的推移,充血性肝病可导致肝桥接纤维化、失代偿性肝硬化和肝细胞癌。目前,尚无针对充血性肝病患的适当筛查或管理的循证指南,部分原因是由于当前的临床工具(血清学检查、影像学研究、肝脏硬度测量和肝活检)无法准确评估肝纤维化或肝失代偿的风险。MELD-XI 评分是唯一经验证的基于血清学的测试,可预测充血性肝病患的临床结局。非侵入性的肝脏硬度测量证明作用不大,因为所有充血性肝病患的数值均升高,但目前无法区分充血和纤维化。此外,由于充血性肝病存在异质性胶原沉积,肝活检进行纤维化分期较难标准化。此外,肝活检结果对于充血性肝病患的心脏移植后肝脏结局的预测价值有限。评估肝结节和肿块在充血性肝病中也很复杂,因为在充血的肝脏背景下,结节内静脉延迟排空的发现并不特异于肝细胞癌,这些病变可能需要活检来确诊。缺乏有效的预测肝纤维化和肝功能的临床工具表明,需要在充血性肝病患中开发新的生物标志物来协助管理这种复杂疾病。(《肝脏病学》2018 年;00:000-000)。