Legemate Catherine M, Goei Harold, Middelkoop Esther, Oen Irma M M H, Nijhuis Tim H J, Kwa Kelly A A, van Zuijlen Paul P M, Beerthuizen Gerard I J M, Nieuwenhuis Marianne K, van Baar Margriet E, van der Vlies Cornelis H
Association of Dutch Burn Centers, Maasstad Hospital, Rotterdam, the Netherlands.
Department of Plastic, Reconstructive and Hand Surgery, Amsterdam Movement Sciences, VU University Medical Center, Amsterdam, the Netherlands.
Trials. 2018 Apr 19;19(1):239. doi: 10.1186/s13063-018-2599-2.
Deep dermal burns require tangential excision of non-viable tissue and skin grafting to improve wound healing and burn-scar quality. Tangential excision is conventionally performed with a knife, but during the last decade hydrosurgery has become popular as a new tool for tangential excision. Hydrosurgery is generally thought to be a more precise and controlled manner of burn debridement leading to preservation of viable tissue and, therefore, better scar quality. Although scar quality is considered to be one of the most important outcomes in burn surgery today, no randomized controlled study has compared the effect of these two common treatment modalities with scar quality as a primary outcome. The aim of this study is, therefore, to compare long-term scar quality after hydrosurgical versus conventional tangential excision in deep dermal burns.
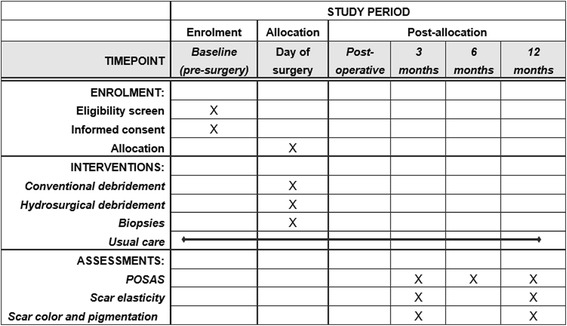
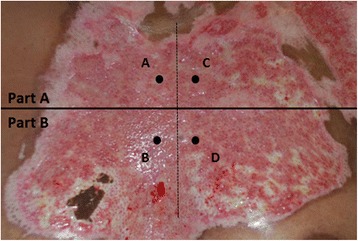
METHODS/DESIGN: A multicenter, randomized, intra-patient, controlled trial will be conducted in the Dutch burn centers of Rotterdam, Beverwijk, and Groningen. All patients with deep dermal burns that require excision and grafting are eligible. Exclusion criteria are: a burn wound < 50 cm, total body surface area (TBSA) burned > 30%, full-thickness burns, chemical or electrical burns, infected wounds (clinical symptoms in combination with positive wound swabs), insufficient knowledge of the Dutch or English language, patients that are unlikely to comply with requirements of the study protocol and follow-up, and patients who are (temporarily) incompetent because of sedation and/or intubation. A total of 137 patients will be included. Comparable wound areas A and B will be appointed, randomized and either excised conventionally with a knife or with the hydrosurgery system. The primary outcome is scar quality measured by the observer score of the Patient and Observer Scar Assessment Scale (POSAS); a subjective scar-assessment instrument, consisting of two separate six-item scales (observer and patient) that are both scored on a 10-point rating scale.
This study will contribute to the optimal surgical treatment of patients with deep dermal burn wounds.
Dutch Trial Register, NTR6232 . Registered on 23 January 2017.
深度真皮烧伤需要对无活力组织进行削痂并植皮,以促进伤口愈合并改善烧伤瘢痕质量。传统上,削痂是用手术刀进行的,但在过去十年中,水刀手术已成为削痂的一种新工具并受到欢迎。一般认为,水刀手术是一种更精确、可控的烧伤清创方式,能保留有活力的组织,因此瘢痕质量更好。尽管瘢痕质量被认为是当今烧伤手术最重要的结果之一,但尚无随机对照研究比较这两种常见治疗方式对瘢痕质量的影响,并将其作为主要结果。因此,本研究的目的是比较水刀手术与传统削痂术后深度真皮烧伤的长期瘢痕质量。
方法/设计:将在荷兰鹿特丹、贝弗维克和格罗宁根的烧伤中心进行一项多中心、随机、患者自身对照试验。所有需要进行削痂和植皮的深度真皮烧伤患者均符合条件。排除标准为:烧伤创面<50平方厘米、烧伤总面积(TBSA)>30%、全层烧伤、化学或电烧伤、感染伤口(临床症状并伴有伤口拭子阳性)、荷兰语或英语知识不足、不太可能遵守研究方案和随访要求的患者,以及因镇静和/或插管(暂时)无行为能力的患者。总共将纳入137例患者。将指定、随机分配可比的伤口区域A和B,分别用手术刀或水刀手术系统进行传统削痂。主要结果是通过患者和观察者瘢痕评估量表(POSAS)的观察者评分来衡量的瘢痕质量;这是一种主观瘢痕评估工具,由两个独立的六项量表(观察者和患者)组成,均采用10分制评分。
本研究将有助于对深度真皮烧伤创面患者进行最佳手术治疗。
荷兰试验注册中心,NTR6232。于2017年1月23日注册。