Picardi Angelo, Fonzi Laura, Pallagrosi Mauro, Gigantesco Antonella, Biondi Massimo
Centre of Behavioural Sciences and Mental Health, Italian National Institute of Health, Rome, Italy.
Department of Human Neurosciences, Sapienza University of Rome, Rome, Italy.
Front Psychiatry. 2018 Apr 5;9:132. doi: 10.3389/fpsyt.2018.00132. eCollection 2018.
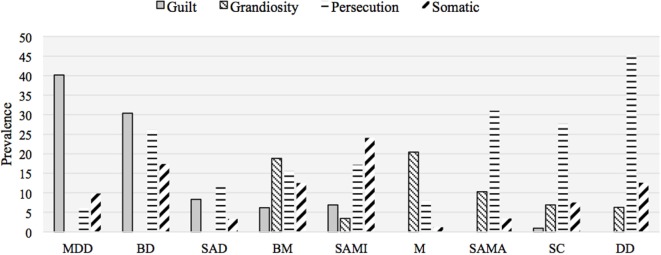
The current debate about the diagnostic significance of delusion revolves around two positions. The neurocognitive position conceives delusion as a non-specific, though polymorphic, symptom. The psychopathological position views features of delusion such as content and structure as having meaningful connections with diagnostic entities. This study aims at contributing to this debate by examining the association between delusional themes and diagnosis in a sample of 830 adult psychotic patients. All diagnoses were made by experienced psychiatrists according to DSM-IV or ICD-10 criteria, and in 348 patients were established with the SCID-I. All patients were administered the Brief Psychiatric Rating Scale (BPRS). In each patient, the presence of somatic delusions and delusions of guilt, grandiosity, and persecution was determined by examining the scores on relevant BPRS items. Delusions of guilt were almost pathognomonic for a psychotic depressive condition (psychotic major depression 40%; psychotic bipolar depression 30%; depressed schizoaffective disorder 8%; bipolar and schizoaffective mixed states 6 and 7%, respectively). Only 1% of patients with schizophrenia and no patient with delusional disorder or bipolar or schizoaffective manic state showed such delusions. The difference between unipolar and bipolar depression and the other diagnostic groups was highly significant. Delusions of grandiosity characterized mostly patients with manic symptoms (bipolar mania 20%; bipolar mixed states 19%; manic schizoaffective disorder 10%). They were observed significantly more often in bipolar mania than in schizophrenia (7%). Persecutory delusions were broadly distributed across diagnostic categories. However, they were significantly more frequent among patients with schizophrenia and delusional disorder compared with depressed and manic patients. Somatic delusions were also observed in all diagnostic groups, with no group standing out as distinct from the others in terms of an increased prevalence of somatic delusions. Our findings suggest a middle position in the debate between the neurocognitive and the psychopathological approaches. On the one hand, the widespread observation of persecutory delusions suggests the usefulness of searching for non-specific pathogenic mechanisms. On the other hand, the association between some delusional contents and psychiatric diagnosis suggests that a phenomenological analysis of the delusional experience may be a helpful tool for the clinician in the diagnostic process.
当前关于妄想诊断意义的争论主要围绕两种观点展开。神经认知观点认为妄想是一种非特异性的症状,尽管具有多形性。心理病理学观点则认为,妄想的特征,如内容和结构,与诊断实体存在有意义的联系。本研究旨在通过调查830名成年精神病患者样本中妄想主题与诊断之间的关联,为这场争论提供参考。所有诊断均由经验丰富的精神科医生根据《精神疾病诊断与统计手册》第四版(DSM-IV)或《国际疾病分类》第十版(ICD-10)标准做出,其中348名患者通过《精神疾病诊断访谈问卷》第一版(SCID-I)确诊。所有患者均接受了简明精神病评定量表(BPRS)评估。在每位患者中,通过检查BPRS相关项目的得分来确定是否存在躯体妄想以及罪恶妄想、夸大妄想和被害妄想。罪恶妄想几乎是精神病性抑郁状态的特征性表现(精神病性重度抑郁为40%;精神病性双相抑郁为30%;抑郁型分裂情感障碍为8%;双相和分裂情感混合状态分别为6%和7%)。精神分裂症患者中只有1%出现此类妄想,妄想性障碍患者、双相或分裂情感性躁狂状态患者均未出现。单相抑郁和双相抑郁与其他诊断组之间的差异极为显著。夸大妄想主要见于有躁狂症状的患者(双相躁狂为20%;双相混合状态为19%;躁狂型分裂情感障碍为10%)。双相躁狂患者中出现夸大妄想的比例显著高于精神分裂症患者(7%)。被害妄想在各诊断类别中分布广泛。然而,与抑郁和躁狂患者相比,精神分裂症和妄想性障碍患者中被害妄想更为常见。所有诊断组中均观察到躯体妄想,在躯体妄想患病率方面,没有一组明显高于其他组。我们的研究结果表明,在神经认知方法和心理病理学方法的争论中应采取中间立场。一方面,被害妄想的广泛存在表明寻找非特异性致病机制是有意义的。另一方面,某些妄想内容与精神科诊断之间的关联表明,对妄想体验进行现象学分析可能有助于临床医生进行诊断。