Moresco Benjamin Louis, Woosley Clinton, Sauter Morris, Bhalala Utpal
Baylor College of Medicine, Houston, TX, United States.
The Children's Hospital of San Antonio, San Antonio, TX, United States.
Front Pediatr. 2018 Apr 5;6:53. doi: 10.3389/fped.2018.00053. eCollection 2018.
This study aimed to assess factors related to adherence to the Pediatric Advanced Life Support guidelines for severe sepsis and septic shock in an emergency room (ER) of a tertiary care children's hospital.
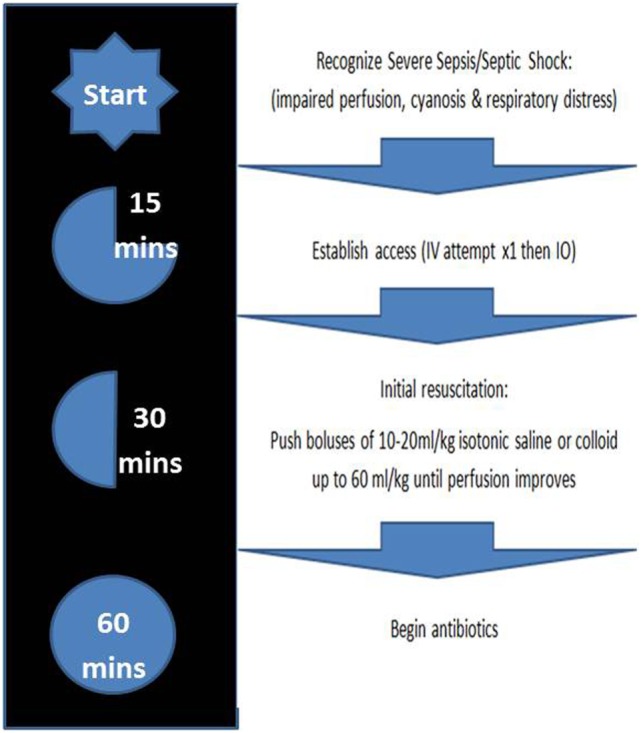
This was a retrospective, observational study of children (0-18 years old) in The Children's Hospital of San Antonio ER over 1 year with the International Consensus Definition Codes, version-9 (ICD-9) diagnostic codes for "severe sepsis" and "shocks." Patients in the adherent group were those who met all three elements of adherence: (1) rapid vascular access with at most one IV attempt before seeking alternate access (unless already in place), (2) fluids administered within 15 min from sepsis recognition, and (3) antibiotic administration started within 1 h of sepsis recognition. Comparisons between groups with and without sepsis guideline adherence were performed using Student's -test (the measurements expressed as median values). The proportions were compared using chi-square test. -Value ≤0.05 was considered significant.
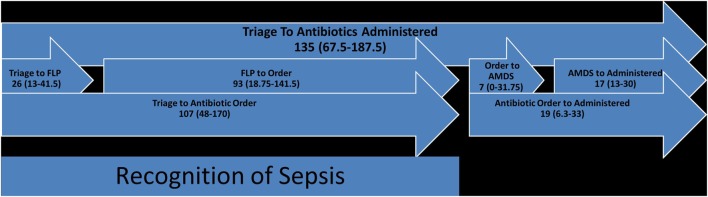
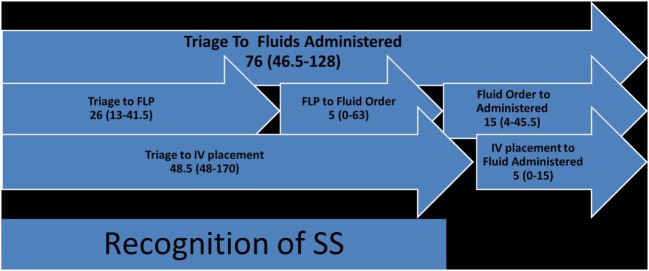
A total of 43 patients who visited the ER from July 2014 to July 2015 had clinically proven severe sepsis or SS ICD-9 codes. The median age was 5 years. The median triage time, times from triage to vascular access, fluid administration and antibiotic administration were 26, 48.5, 76, and 135 min, respectively. Adherence to vascular access, fluid, and antibiotic administration guidelines was 21, 26, and 34%, respectively. Appropriate fluid bolus (20 ml/kg over 15-20 min) was only seen in 6% of patients in the non-adherent group versus 38% in the adherent group ( = 0.01). All of the patients in the non-adherent group used an infusion pump for fluid resuscitation. Hypotension and ≥3 organ dysfunction were more commonly observed in patients in adherent group as compared to patients in non-adherent group (38 vs. 14% = 0.24; 63 vs. 23% = 0.03).
Overall adherence to sepsis guidelines was low. The factors associated with non-adherence to sepsis guidelines were >1 attempt at vascular access, delay in antibiotic ordering, fluid administration using infusion pump, absence of hypotension, and absence of three or more organs in dysfunction at ER presentation.
本研究旨在评估一家三级儿童专科医院急诊科中与严重脓毒症和脓毒性休克患者遵循儿科高级生命支持指南相关的因素。
这是一项对圣安东尼奥儿童医院急诊科1年内0至18岁儿童进行的回顾性观察研究,采用国际共识定义编码第9版(ICD - 9)中“严重脓毒症”和“休克”的诊断编码。遵循指南组患者是指符合所有三项遵循要素的患者:(1)快速建立血管通路,在寻求其他通路之前最多进行一次静脉穿刺尝试(除非已建立);(2)在识别脓毒症后15分钟内给予液体;(3)在识别脓毒症后1小时内开始使用抗生素。对遵循和未遵循脓毒症指南的两组进行比较时,采用学生t检验(测量值以中位数表示)。比例比较采用卡方检验。P值≤0.05被认为具有统计学意义。
2014年7月至2015年7月期间,共有43名到急诊科就诊且临床确诊为严重脓毒症或脓毒性休克的患者有ICD - 9编码。中位年龄为5岁。中位分诊时间、从分诊到建立血管通路、给予液体和使用抗生素的时间分别为26、48.5、76和135分钟。血管通路、液体和抗生素使用指南的遵循率分别为21%、26%和34%。非遵循组中仅6%的患者给予了适当的液体冲击量(15至20分钟内20 ml/kg),而遵循组为38%(P = 0.01)。非遵循组的所有患者均使用输液泵进行液体复苏。与非遵循组患者相比,遵循组患者更常出现低血压和≥3个器官功能障碍(38%对14%,P = 0.24;63%对23%,P = 0.03)。
脓毒症指南的总体遵循率较低。与未遵循脓毒症指南相关的因素包括血管穿刺尝试超过1次、抗生素医嘱延迟、使用输液泵给予液体、无低血压以及急诊科就诊时无3个或更多器官功能障碍。