Jaffal Karim, Poissy Julien, Rouze Anahita, Preau Sébastien, Sendid Boualem, Cornu Marjorie, Nseir Saad
Critical Care Center, CHU Lille, 59000, Lille, France.
U995-LIRIC-Lille Inflammation Research International Center, Univ. Lille, 59000, Lille, France.
Ann Intensive Care. 2018 Apr 19;8(1):49. doi: 10.1186/s13613-018-0392-8.
Antifungal treatment is common in critically ill patients, but only a small proportion of patients receiving antifungals have a proven fungal infection. However, antifungal treatment has side effects such as toxicity, emergence of resistance, and high cost. Moreover, empirical antifungal treatment is still a matter for debate in these patients. Our study aimed to determine the incidence, associated factors, and safety of de-escalation of antifungals in critically ill patients.
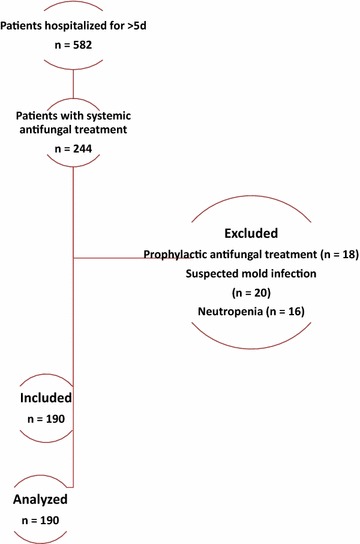
This retrospective study was conducted in a 30-bed mixed ICU, from January 2012 through January 2013. Patients hospitalized for > 5 days and treated with antifungals for first suspected or proven invasive Candida infection were included. Exclusion criteria were prophylactic antifungals, suspected invasive aspergillosis, and neutropenia. De-escalation was defined as switch from initial systemic antifungals (except fluconazole) to triazoles, or stopping initial drugs within the 5 days following their initiation.
One hundred and ninety patients were included. Antifungal treatment was empirical, preemptive, and targeted in 55, 27, and 24% of study patients, respectively. Caspofungin (53%), fluconazole (43%), voriconazole (4%), and liposomal amphotericin B (0.5%) were the more frequently used antifungals. De-escalation was performed in 38 (20%) patients. Invasive mechanical ventilation was independently associated with lower rates of de-escalation (OR 0.25 [95% CI 0.08-0.85], p = 0.013). Total duration of antifungal treatment was significantly shorter in patients with de-escalation, compared with those with no de-escalation (med [IQR] 6 (5, 18) vs. 13 days (7, 25), p = 0.023). No significant difference was found in duration of mechanical ventilation (22 [5-31] vs. 20 days [10-35], p = 0.43), length of ICU stay (25 [14-40) vs. 25 days [11-40], p = 0.99), ICU mortality (45 vs. 59%, p = 0.13), or 1-year mortality (55 vs. 64%, p = 0.33) between patients with de-escalation and those with no de-escalation, respectively.
De-escalation was performed in 20% of patients receiving systemic antifungals for suspected or proven invasive Candida infection. Mechanical ventilation was independently associated with lower rates of de-escalation. De-escalation of antifungal treatment seems to be safe in critically ill patients.
抗真菌治疗在重症患者中很常见,但接受抗真菌治疗的患者中只有一小部分被证实有真菌感染。然而,抗真菌治疗有副作用,如毒性、耐药性的出现和高成本。此外,经验性抗真菌治疗在这些患者中仍然存在争议。我们的研究旨在确定重症患者抗真菌药物降阶梯治疗的发生率、相关因素和安全性。
这项回顾性研究于2012年1月至2013年1月在一个有30张床位的混合重症监护病房进行。纳入住院超过5天且因首次怀疑或证实的侵袭性念珠菌感染接受抗真菌治疗的患者。排除标准为预防性抗真菌治疗、疑似侵袭性曲霉病和中性粒细胞减少症。降阶梯治疗定义为从初始全身性抗真菌药物(氟康唑除外)转换为三唑类药物,或在初始药物开始使用后的5天内停用初始药物。
共纳入190例患者。抗真菌治疗分别在55%、27%和24%的研究患者中为经验性、抢先性和靶向性治疗。卡泊芬净(53%)、氟康唑(43%)、伏立康唑(4%)和脂质体两性霉素B(0.5%)是使用较频繁的抗真菌药物。38例(20%)患者进行了降阶梯治疗。有创机械通气与较低的降阶梯治疗率独立相关(比值比0.25 [95%可信区间0.08 - 0.85],p = 0.013)。与未进行降阶梯治疗的患者相比,进行降阶梯治疗的患者抗真菌治疗的总持续时间显著缩短(中位数[四分位间距]6(5,18)天对13天(7,25)天,p = 0.023)。在机械通气持续时间(22 [5 - 31]天对20天[10 - 35]天,p = 不显著差异0.43)、重症监护病房住院时间(25 [14 - 40]天对25天[11 - 40]天,p = 0.99)、重症监护病房死亡率(45%对59%,p = 0.13)或1年死亡率(55%对64%,p = 0.33)方面,进行降阶梯治疗的患者与未进行降阶梯治疗的患者之间均未发现显著差异。
在因疑似或证实的侵袭性念珠菌感染接受全身性抗真菌治疗的患者中,20%的患者进行了降阶梯治疗。机械通气与较低的降阶梯治疗率独立相关。抗真菌治疗的降阶梯在重症患者中似乎是安全的。