Tonolini Massimo, Ierardi Anna Maria, Carrafiello Gianpaolo, Laganà Domenico
Department of Radiology, "Luigi Sacco" University Hospital, Via G.B. Grassi 74, 20157, Milan, Italy.
Diagnostic and Interventional Radiology Department, ASST Santi Paolo e Carlo, Via A di Rudinì 8, 20142, Milan, Italy.
Insights Imaging. 2018 Aug;9(4):631-642. doi: 10.1007/s13244-018-0613-6. Epub 2018 Apr 19.
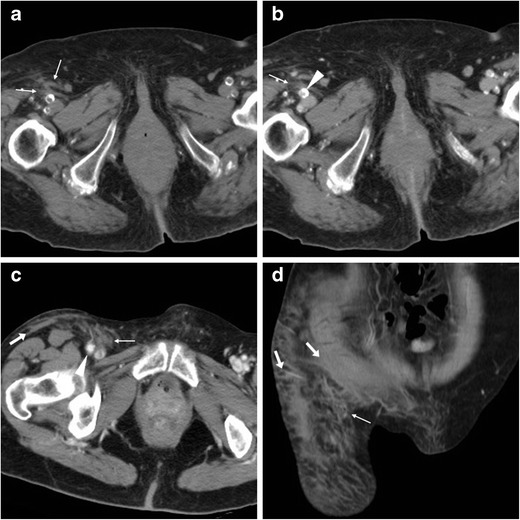
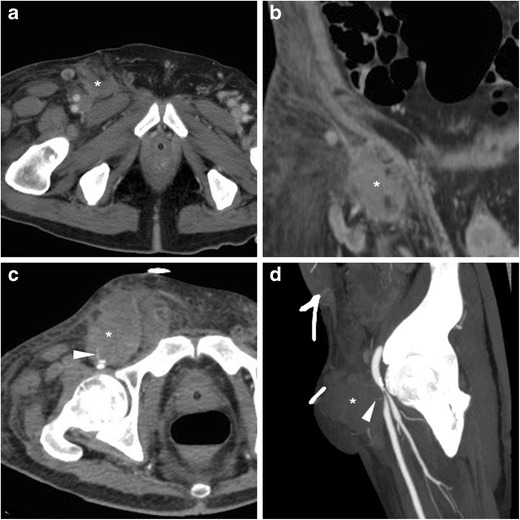
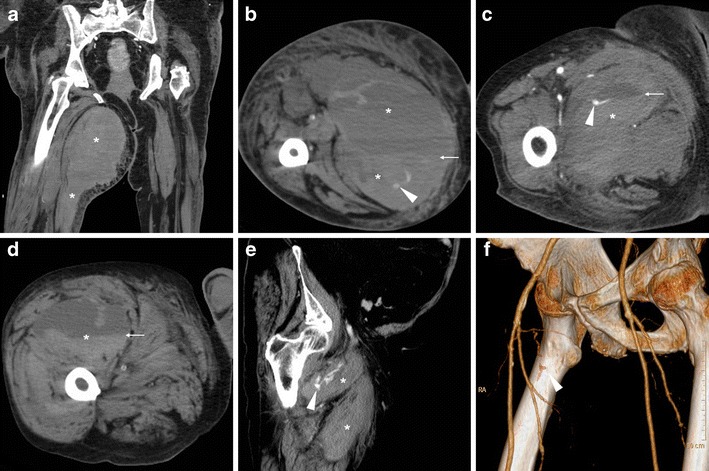
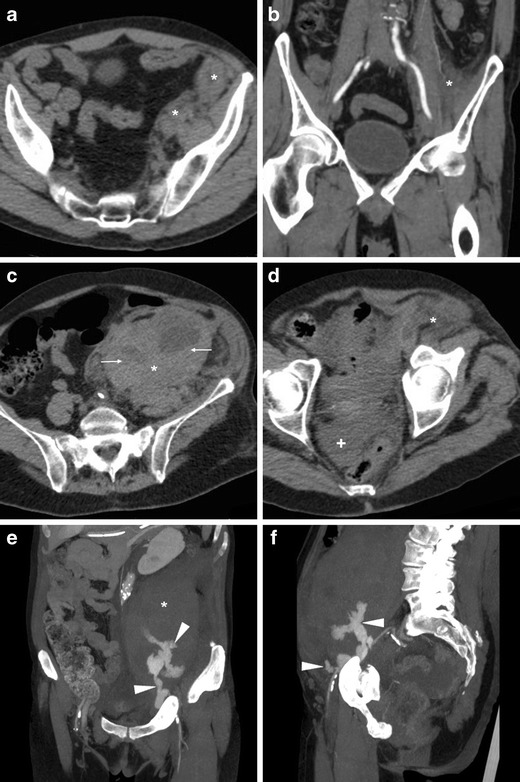
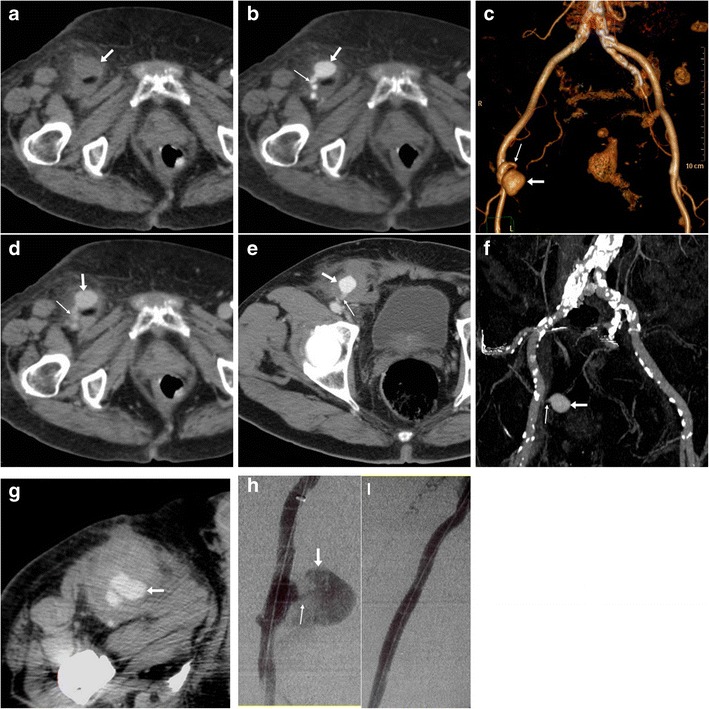
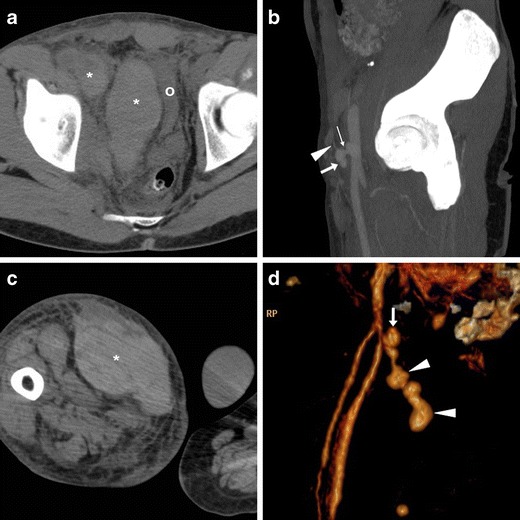
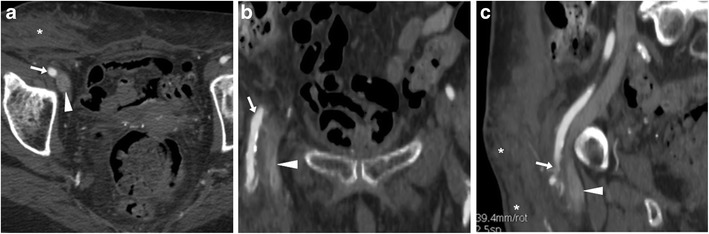
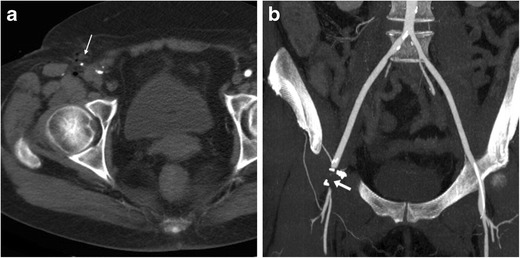
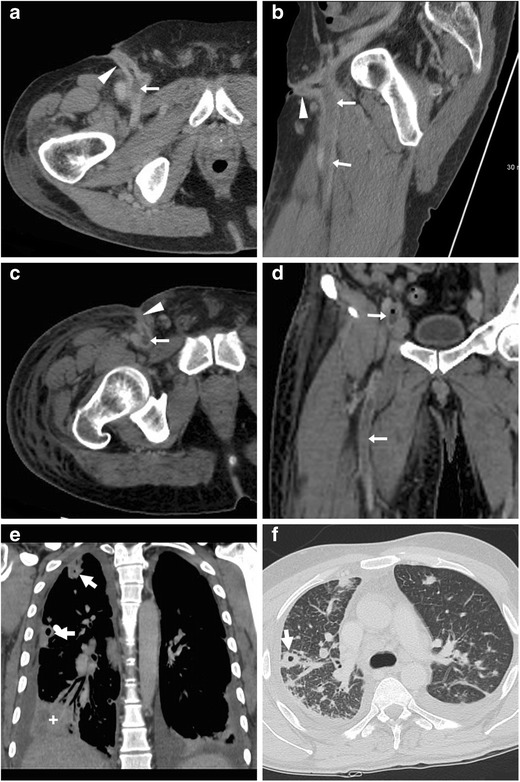
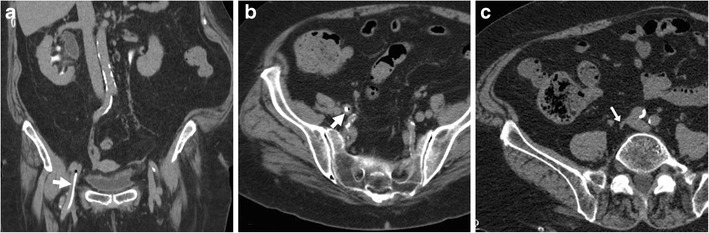
The number and complexity of endovascular procedures performed via either arterial or venous access are steadily increasing. Albeit associated with higher morbidity compared to the radial approach, the traditional common femoral artery remains the preferred access site in a variety of cardiac, aortic, oncologic and peripheral vascular procedures. Both transarterial and venous cannulation (for electrophysiology, intravenous laser ablation and central catheterisation) at the groin may result in potentially severe vascular access site complications (VASC). Furthermore, vascular and soft-tissue groin infections may develop after untreated VASC or secondarily to non-sterile injections for recreational drug use. VASC and groin infections require rapid diagnosis and appropriate treatment to avoid further, potentially devastating harm. Whereas in the past colour Doppler ultrasound was generally used, in recent years cardiologists, vascular surgeons and interventional radiologists increasingly rely on pelvic and femoral CT angiography. Despite drawbacks of ionising radiation and the need for intravenous contrast, multidetector CT rapidly and consistently provides a panoramic, comprehensive visualisation, which is crucial for correct choice between conservative, endovascular and surgical management. This paper aims to provide radiologists with an increased familiarity with iatrogenic and self-inflicted VASC and infections at the groin by presenting examples of haematomas, active bleeding, pseudoaneurysms, arterial occlusion, arterio-venous fistula, endovenous heat-induced thrombosis, septic thrombophlebitis, soft-tissue infections at the groin, and late sequelae of venous injuries.
• Complications may develop after femoral arterial or venous access for interventional procedures. • Arterial injuries include bleeding, pseudoaneurysm, occlusion, arteriovenous fistula, dissection. • Endovenous heat-induced thrombosis is a specific form of iatrogenic venous complication. • Iatrogenic infections include groin cellulitis, abscesses and septic thrombophlebitis. • CT angiography reliably triages vascular access site complications and groin infections.
通过动脉或静脉入路进行的血管内手术的数量和复杂性正在稳步增加。尽管与桡动脉入路相比,传统的股总动脉入路的发病率更高,但在各种心脏、主动脉、肿瘤和外周血管手术中,它仍然是首选的入路部位。腹股沟处的经动脉和静脉插管(用于电生理、静脉激光消融和中心静脉置管)都可能导致潜在的严重血管入路部位并发症(VASC)。此外,未经治疗的VASC或继发于非无菌娱乐性药物注射后,可能会发生血管和软组织腹股沟感染。VASC和腹股沟感染需要快速诊断和适当治疗,以避免进一步的、可能具有毁灭性的伤害。过去一般使用彩色多普勒超声,近年来,心脏病专家、血管外科医生和介入放射科医生越来越依赖盆腔和股部CT血管造影。尽管存在电离辐射的缺点以及需要静脉注射造影剂,但多排CT能快速、一致地提供全景、全面的可视化图像,这对于在保守治疗、血管内治疗和手术治疗之间做出正确选择至关重要。本文旨在通过展示血肿、活动性出血、假性动脉瘤、动脉闭塞、动静脉瘘、静脉内热诱导血栓形成、感染性血栓性静脉炎、腹股沟软组织感染以及静脉损伤的晚期后遗症等实例,使放射科医生更熟悉腹股沟处医源性和自伤性VASC及感染。
• 介入手术的股动脉或静脉入路后可能会出现并发症。• 动脉损伤包括出血、假性动脉瘤、闭塞、动静脉瘘、夹层。• 静脉内热诱导血栓形成是医源性静脉并发症的一种特殊形式。• 医源性感染包括腹股沟蜂窝织炎、脓肿和感染性血栓性静脉炎。• CT血管造影能可靠地对血管入路部位并发症和腹股沟感染进行分类。