Bakhshayesh Peyman, Weidenhielm Lars, Enocson Anders
Department of Molecular Medicine and Surgery (MMK), Karolinska Institute, 17176, Stockholm, Sweden.
Eur J Orthop Surg Traumatol. 2018 Oct;28(7):1273-1282. doi: 10.1007/s00590-018-2203-1. Epub 2018 Apr 19.
Factors affecting mortality during the first year following high-energy pelvic fractures has not been reported previously. Nor has surgical complications leading to reoperations been reported in a cohort with only high-energy pelvic trauma patients.
The aim of this study was to report and analyse factors affecting outcome, in terms of mortality and reoperations, up to 1 year after the injury in patients with a traumatic pelvic ring injury due to a high-energy trauma.
Data from the SweTrau (Swedish National Trauma Registry) on patients admitted to the Trauma Centre Karolinska in Stockholm, Sweden, were collected. Inclusion criteria were adults (age ≥ 18), trauma with a high-energy mechanism, alive on arrival, Swedish personal identification number, reported pelvic fracture on CT scan. Patient records and radiographies were reviewed. The study period was 2011-2015 with 1-year follow-up time. Univariate and regression analysis on factors affecting mortality was performed. Risk of reoperation was analysed using univariate and case-by-case analysis.
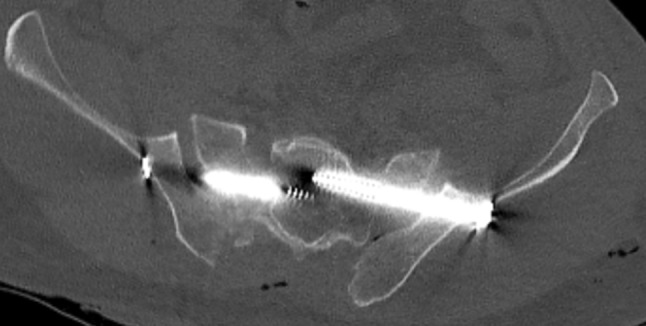
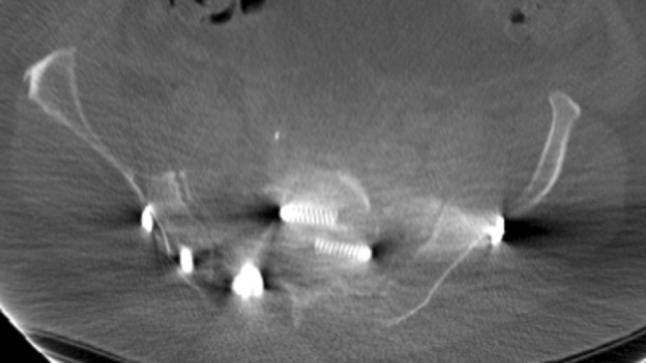
We included 385 cases with mean age 47.5 ± 20.6 years (38% females): 317 pelvic fractures, 48 acetabular fractures and 20 combined injuries. Thirty-day mortality was 8% (30/385), and 1-year mortality was 9% (36/385). The main cause of death at 1 year was traumatic brain injury (14/36) followed by high age (> 70) with extensive comorbidities (8/36). Intentional fall from high altitude (OR 6, CI 2-17), GCS < 8 (OR 12, CI 5-33) and age > 70 (OR 17, CI 6-51) were factors predicting mortality. Thirty patients (22%, 30/134) were further reoperated due to hardware-related (n = 18) or non-hardware-related complications (n = 12). Hardware-related complications included: mal-placed screws (n = 7), mal-placed plate (n = 1), implant failure (n = 6), or mechanical irritation from the implant (n = 4). Non-hardware-related reasons for reoperations were: infection (n = 10), skin necrosis (n = 1), or THR due to post-traumatic osteoarthritis (n = 1).
Non-survivors in our study died mainly because of traumatic brain injury or high age with extensive comorbidities. Most of the mortalities occurred early. Intentional injuries and especially intentional falls from high altitude had high mortality rate. Reoperation frequency was high, and several of the hardware-related complications could potentially have been avoided.
此前尚未报道过高能量骨盆骨折后第一年的死亡影响因素。在仅包含高能量骨盆创伤患者的队列中,也未报道过导致再次手术的手术并发症。
本研究的目的是报告并分析高能创伤导致创伤性骨盆环损伤患者受伤后长达1年的死亡率和再次手术等影响预后的因素。
收集瑞典国家创伤登记处(SweTrau)中瑞典斯德哥尔摩卡罗林斯卡创伤中心收治患者的数据。纳入标准为成年人(年龄≥18岁)、高能机制创伤、入院时存活、有瑞典个人身份识别号码、CT扫描报告有骨盆骨折。回顾患者记录和X光片。研究期间为2011 - 2015年,随访时间为1年。对影响死亡率的因素进行单因素分析和回归分析。使用单因素分析和逐例分析来分析再次手术的风险。
我们纳入了385例患者,平均年龄47.5±20.6岁(38%为女性):317例骨盆骨折、48例髋臼骨折和20例复合伤。30天死亡率为8%(30/385),1年死亡率为9%(36/385)。1年时的主要死亡原因是创伤性脑损伤(14/36),其次是高龄(>70岁)且有多种合并症(8/36)。从高处故意坠落(比值比6,可信区间2 - 17)、格拉斯哥昏迷评分<8分(比值比12,可信区间5 - 33)和年龄>70岁(比值比17,可信区间6 - 51)是预测死亡率的因素。30例患者(22%,30/134)因硬件相关(n = 18)或非硬件相关并发症(n = 12)而再次手术。硬件相关并发症包括:螺钉位置不当(n = 7)、钢板位置不当(n = 1)、植入物失效(n = 6)或植入物机械刺激(n = 4)。再次手术的非硬件相关原因包括:感染(n = 10)、皮肤坏死(n = 1)或创伤后骨关节炎导致的全髋关节置换术(n = 1)。
我们研究中的非幸存者主要死于创伤性脑损伤或高龄且有多种合并症。大多数死亡发生在早期。故意伤害,尤其是从高处故意坠落,死亡率很高。再次手术频率较高,一些硬件相关并发症可能本可避免。