Division of Hematology, Oncology and Transplantation.
Biostatistics Core, Masonic Cancer Center, and.
Blood Adv. 2018 Apr 24;2(8):909-922. doi: 10.1182/bloodadvances.2017014464.
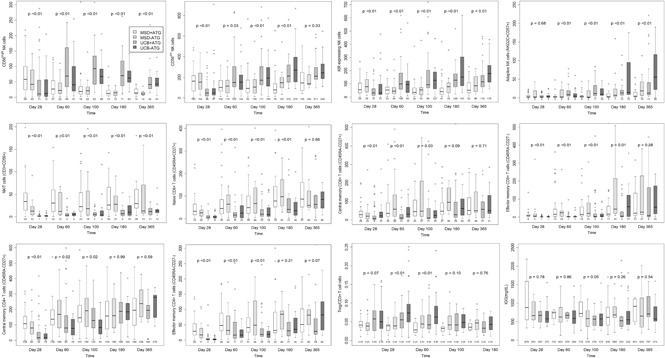
Slow immune reconstitution is a major obstacle to the successful use of allogeneic hematopoietic cell transplantation (allo-HCT). As matched sibling donor (MSD) allo-HCT is regarded as the gold standard, we evaluated the pace of immune reconstitution in 157 adult recipients of reduced-intensity conditioning followed by MSD peripheral blood HCT (n = 68) and compared these to recipients of umbilical cord blood (UCB; n = 89). At day 28, UCB recipients had fewer natural killer (NK) cells than MSD recipients, but thereafter, NK cell numbers (and their subsets) were higher in UCB recipients. During the first 6 months to 1 year after transplant, UCB recipients had slower T-cell subset recovery, with lower numbers of CD3, CD8, CD8 naive, CD4 naive, CD4 effector memory T, regulatory T, and CD3CD56 T cells than MSD recipients. Notably, B-cell numbers were higher in UCB recipients from day 60 to 1 year. Bacterial and viral infections were more frequent in UCB recipients, yet donor type had no influence on treatment-related mortality or survival. Considering all patients at day 28, lower numbers of total CD4 T cells and naive CD4 T cells were significantly associated with increased infection risk, treatment-related mortality, and chronic graft-versus-host disease (GVHD). Patients with these characteristics may benefit from enhanced or prolonged infection surveillance and prophylaxis as well as immune reconstitution-accelerating strategies.
免疫重建缓慢是异体造血细胞移植(allo-HCT)成功应用的主要障碍。由于匹配的同胞供体(MSD)allo-HCT 被视为金标准,我们评估了 157 例接受低强度预处理后接受 MSD 外周血 HCT(n=68)和接受脐带血(UCB;n=89)的成年受者的免疫重建速度。在第 28 天,UCB 受者的自然杀伤(NK)细胞比 MSD 受者少,但此后 UCB 受者的 NK 细胞数量(及其亚群)更高。在移植后 6 个月至 1 年内,UCB 受者的 T 细胞亚群恢复较慢,CD3、CD8、CD8 幼稚、CD4 幼稚、CD4 效应记忆 T、调节 T 和 CD3CD56 T 细胞数量均低于 MSD 受者。值得注意的是,从第 60 天到 1 年,UCB 受者的 B 细胞数量较高。UCB 受者的细菌和病毒感染更为频繁,但供体类型对治疗相关死亡率或生存率没有影响。考虑到所有患者在第 28 天,总 CD4 T 细胞和幼稚 CD4 T 细胞数量较少与感染风险增加、治疗相关死亡率和慢性移植物抗宿主病(GVHD)显著相关。具有这些特征的患者可能受益于增强或延长感染监测和预防以及免疫重建加速策略。