Nyakato Patience, Kiragga Agnes N, Kambugu Andrew, Bradley John, Baisley Kathy
MRC Tropical Epidemiology Group, Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK.
Infectious Diseases Institute, College of Health Sciences, Makerere University, Kampala, Uganda.
BMJ Open. 2018 Apr 20;8(4):e017487. doi: 10.1136/bmjopen-2017-017487.
The aim of this study was to use a sampling-based approach to obtain estimates of retention in HIV care before initiation of antiretroviral treatment (ART), corrected for outcomes in patients who were lost according to clinic registers.
Retrospective cohort study of HIV-positive individuals not yet eligible for ART (CD4 >500).
Three urban and three rural HIV care clinics in Uganda; information was extracted from the clinic registers for all patients who had registered for pre-ART care between January and August 2015.
A random sample of patients who were lost according to the clinic registers (>3 months late to scheduled visit) was traced to ascertain their outcomes.
The proportion of patients lost from care was estimated using a competing risks approach, first based on the information in the clinic records alone and then using inverse probability weights to incorporate the results from tracing. Cox regression was used to determine factors associated with loss from care.
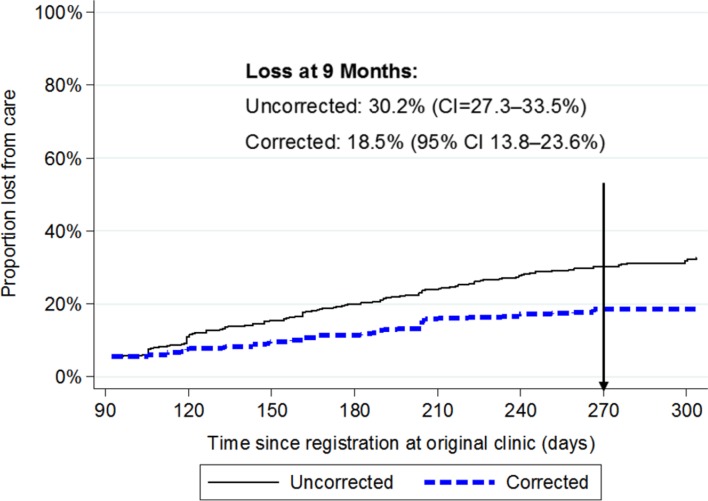
Of 1153 patients registered for pre-ART care (68% women, median age 29 years, median CD4 count 645 cells/µL), 307 (27%) were lost according to clinic records. Among these, 195 (63%) were selected for tracing; outcomes were ascertained in 118 (61%). Seven patients (6%) had died, 40 (34%) were in care elsewhere and 71 (60%) were out of care. Loss from care at 9 months was 30.2% (95% CI 27.3% to 33.5%). After incorporating outcomes from tracing, loss from care decreased to 18.5% (95% CI 13.8% to 23.6%).
Estimates of loss from HIV care may be too high if based on routine clinic data alone. A sampling-based approach is a feasible way of obtaining more accurate estimates of retention, accounting for transfers to other clinics.
本研究旨在采用基于抽样的方法,在开始抗逆转录病毒治疗(ART)之前,获取艾滋病病毒(HIV)护理留存率的估计值,并针对根据诊所登记记录失访患者的结局进行校正。
对尚未符合ART治疗条件(CD4>500)的HIV阳性个体进行回顾性队列研究。
乌干达的三家城市和三家农村HIV护理诊所;从2015年1月至8月期间登记接受ART前护理的所有患者的诊所登记记录中提取信息。
根据诊所登记记录失访(预定就诊迟到超过3个月)的患者的随机样本被追踪以确定其结局。
使用竞争风险方法估计失访患者的比例,首先仅基于诊所记录中的信息,然后使用逆概率权重纳入追踪结果。采用Cox回归确定与失访相关的因素。
在1153名登记接受ART前护理的患者中(68%为女性,中位年龄29岁,中位CD4计数645个细胞/微升),根据诊所记录有307名(27%)失访。其中,195名(63%)被选作追踪对象;118名(61%)的结局得以确定。7名患者(6%)死亡,40名(34%)在其他地方接受护理,71名(60%)失访。9个月时的失访率为30.2%(95%置信区间27.3%至33.5%)。纳入追踪结果后,失访率降至18.5%(95%置信区间13.8%至23.6%)。
如果仅基于常规诊所数据,HIV护理失访率的估计可能过高。基于抽样的方法是获得更准确留存率估计值的可行方法,同时考虑到转至其他诊所的情况。