Division of HIV, Infectious Diseases and Global Medicine, Zuckerberg San Francisco General Hospital and Trauma Center, University of California, San Francisco, San Francisco, California, United States of America.
Centre for Infectious Disease Research in Zambia, Lusaka, Zambia.
PLoS Med. 2020 May 13;17(5):e1003107. doi: 10.1371/journal.pmed.1003107. eCollection 2020 May.
Men in sub-Saharan Africa have lower engagement and retention in HIV services compared to women, which may result in differential survival. However, the true magnitude of difference in HIV-related mortality between men and women receiving antiretroviral therapy (ART) is incompletely characterized.
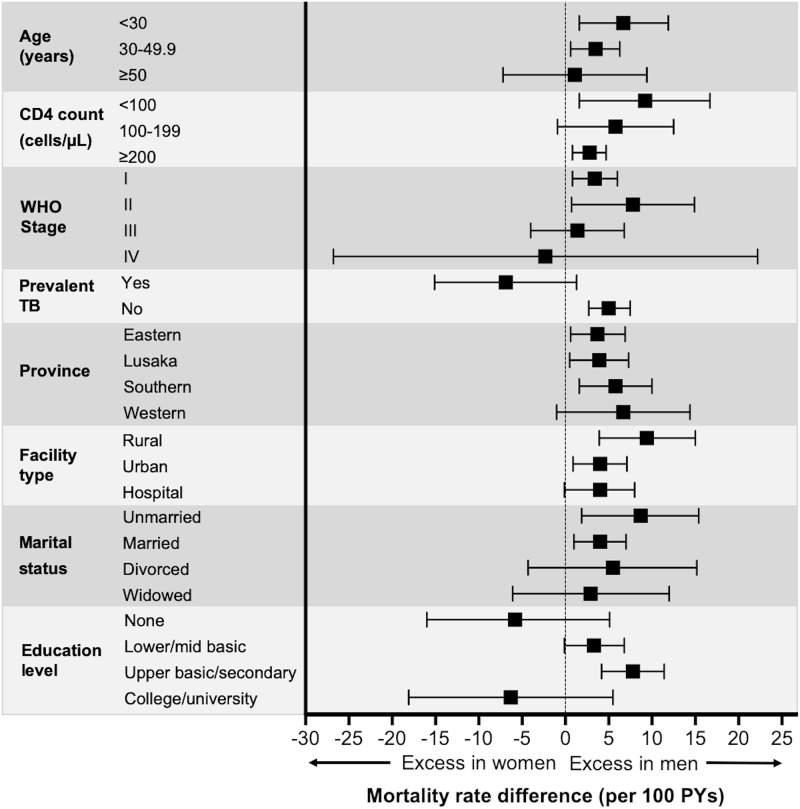
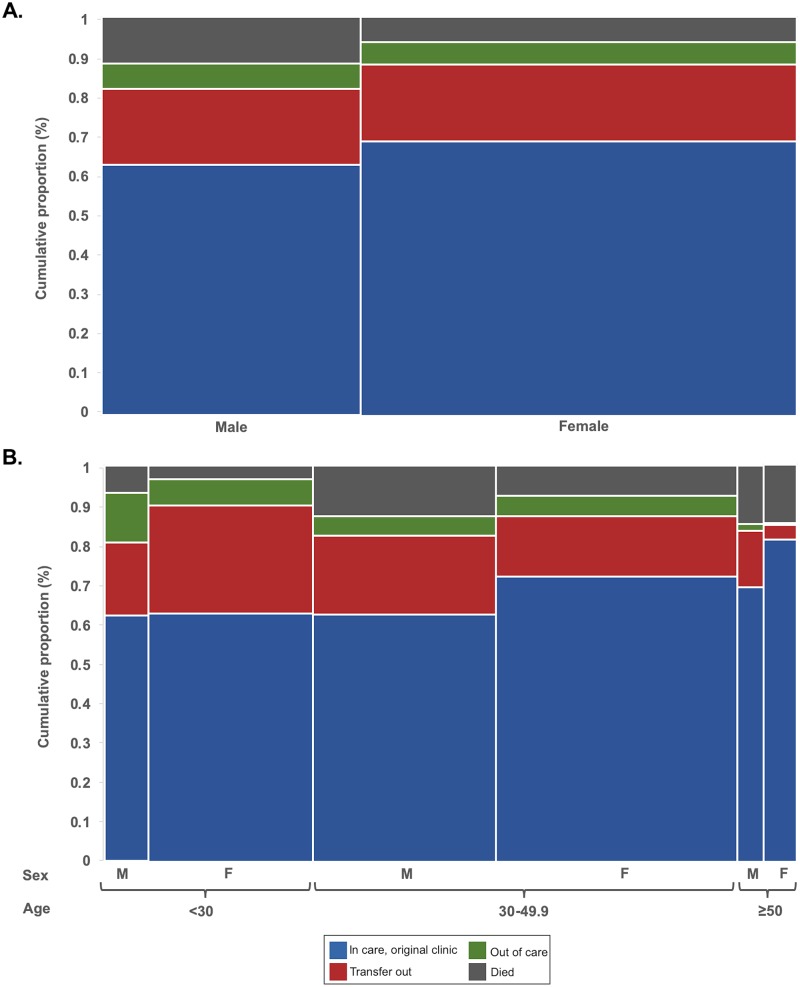
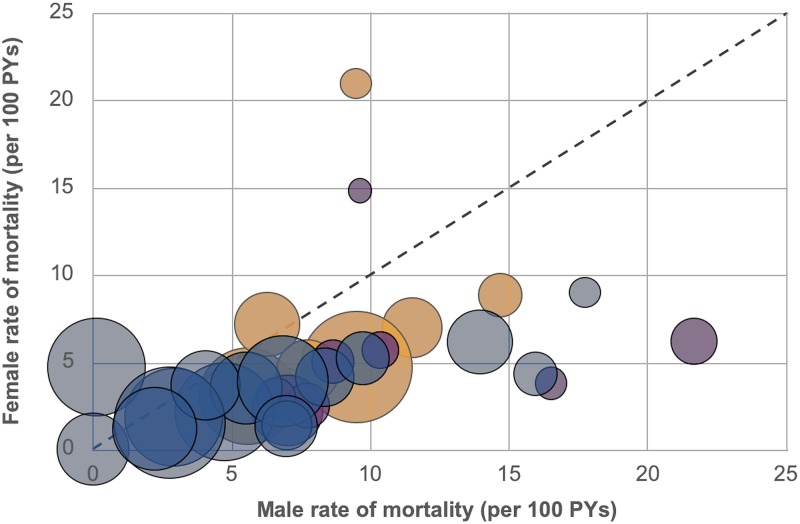
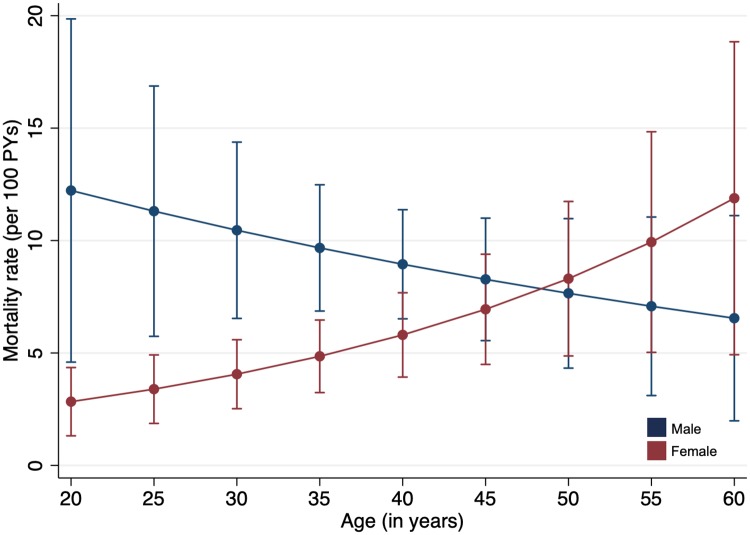
We evaluated HIV-positive adults ≥18 years old newly initiating ART in 4 Zambian provinces (Eastern, Lusaka, Southern, and Western). In addition to mortality data obtained from routine electronic medical records, we intensively traced a random sample of patients lost to follow-up (LTFU) and incorporated tracing outcomes through inverse probability weights. Sex-specific mortality rates and rate differences were determined using Poisson regression. Parametric g-computation was used to estimate adjusted mortality rates by sex and age. The study included 49,129 adults newly initiated on ART between August 2013 and July 2015; overall, the median age among patients was 35 years, the median baseline CD4 count was 262 cells/μl, and 37.2% were men. Men comprised a smaller proportion of individuals starting ART (37.2% versus 62.8%), tended to be older (median age 37 versus 33 years), and tended to have lower CD4 counts (median 220 versus 289 cells/μl) at the time of ART initiation compared to women. The overall rate of mortality among men was 10.3 (95% CI 8.2-12.4) deaths/100 person-years (PYs), compared to 5.5 (95% CI 4.3-6.8) deaths/100 PYs among women (difference +4.7 [95% CI 2.3-7.2] deaths/100 PYs; p < 0.001). Compared to women in the same age groups, men's mortality rates were particularly elevated among those <30 years old (+6.7 deaths/100 PYs difference), those attending rural health centers (+9.4 deaths/100 PYs difference), those who had an initial CD4 count < 100 cells/μl (+9.2 deaths/100 PYs difference), and those who were unmarried (+8.0 deaths/100 PYs difference). After adjustment for potential confounders and mediators including CD4 count, a substantially higher mortality rate was predicted among men <30 years old compared to women of the same age, while women ≥50 years old had a mortality rate similar to that of age-matched men, but considerably higher than that predicted among young women (<30 years old). No clinically significant differences were evident with respect to rates of facility transfer or care disengagement between men and women. The main study limitations were the inability to successfully ascertain outcomes in all patients selected for tracing and missing clinical and laboratory data due to the use of medical records.
In this study, we found that among HIV-positive adults newly initiating ART, mortality among men exceeded mortality among women; disparities were most pronounced among young patients. Older women, however, also experienced high mortality. Specific interventions for men and older women at highest mortality risk are needed to improve HIV treatment outcomes.
与女性相比,撒哈拉以南非洲的男性在参与和保留艾滋病毒服务方面较低,这可能导致生存差异。然而,接受抗逆转录病毒治疗(ART)的男性和女性之间在与艾滋病毒相关的死亡率方面的真实差异程度尚未完全描述。
我们评估了在赞比亚的四个省份(东部、卢萨卡、南部和西部)新开始接受 ART 的≥18 岁的 HIV 阳性成年人。除了从常规电子病历中获得的死亡率数据外,我们还对大量随访丢失(LTFU)的患者进行了跟踪,并通过逆概率权重纳入了跟踪结果。使用泊松回归确定性别特异性死亡率和死亡率差异。使用参数 g 计算估计按性别和年龄调整的死亡率。这项研究包括 2013 年 8 月至 2015 年 7 月期间新开始接受 ART 的 49129 名成年人;总体而言,患者的中位年龄为 35 岁,中位基线 CD4 计数为 262 个细胞/μl,37.2%为男性。与女性相比,开始接受 ART 的男性比例较小(37.2%对 62.8%),年龄较大(中位数 37 岁对 33 岁),并且在开始接受 ART 时 CD4 计数较低(中位数 220 对 289 个细胞/μl)。男性的总死亡率为 10.3(95%CI 8.2-12.4)死亡/100 人年(PYs),而女性为 5.5(95%CI 4.3-6.8)死亡/100 PYs(差异为+4.7[95%CI 2.3-7.2]死亡/100 PYs;p<0.001)。与同年龄组的女性相比,男性的死亡率在<30 岁的人群中尤其升高(差异为+6.7 死亡/100 PYs),在农村卫生中心就诊的人群中(差异为+9.4 死亡/100 PYs),在初始 CD4 计数<100 个细胞/μl 的人群中(差异为+9.2 死亡/100 PYs),以及在未婚的人群中(差异为+8.0 死亡/100 PYs)。在调整了包括 CD4 计数在内的潜在混杂因素和中介因素后,与同年龄的女性相比,<30 岁的男性死亡率明显更高,而≥50 岁的女性死亡率与同龄男性相似,但明显高于年轻女性(<30 岁)的死亡率预测。在男性和女性之间,设施转移或护理脱离的比率没有明显差异。本研究的主要局限性是无法成功确定所有选定用于跟踪的患者的结局,并且由于使用病历,临床和实验室数据缺失。
在这项研究中,我们发现新开始接受抗逆转录病毒治疗的 HIV 阳性成年人中,男性的死亡率高于女性;在年轻患者中差异最为明显。然而,老年女性也经历了较高的死亡率。需要针对高死亡率的男性和老年女性采取具体的干预措施,以改善艾滋病毒治疗结果。