Department of Psychosis Studies, Institute of Psychiatry, Psychology and Neuroscience, King's College, London, UK.
Early Intervention Psychosis Clinical Academic Group, South London & Maudsley NHS Trust, London, UK.
Mol Psychiatry. 2019 Oct;24(10):1502-1512. doi: 10.1038/s41380-018-0042-4. Epub 2018 Apr 20.
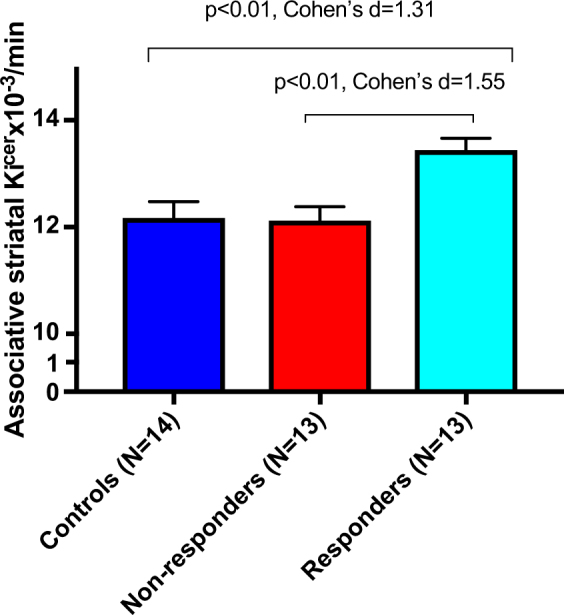
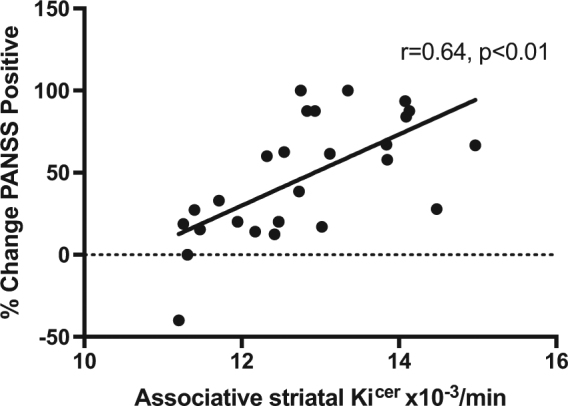
Psychotic illnesses show variable responses to treatment. Determining the neurobiology underlying this is important for precision medicine and the development of better treatments. It has been proposed that dopaminergic differences underlie variation in response, with striatal dopamine synthesis capacity (DSC) elevated in responders and unaltered in non-responders. We therefore aimed to test this in a prospective cohort, with a nested case-control comparison. 40 volunteers (26 patients with first-episode psychosis and 14 controls) received an F-DOPA Positron Emission Tomography scan to measure DSC (Ki) prior to antipsychotic treatment. Clinical assessments (Positive and Negative Syndrome Scale, PANSS, and Global Assessment of Functioning, GAF) occurred at baseline and following antipsychotic treatment for a minimum of 4 weeks. Response was defined using improvement in PANSS Total score of >50%. Patients were followed up for at least 6 months, and remission criteria applied. There was a significant effect of group on Ki in associative striatum (F = 7.9, p = 0.001). Ki was significantly higher in responders compared with non-responders (Cohen's d = 1.55, p = 0.01) and controls (Cohen's d = 1.31, p = 0.02). Ki showed significant positive correlations with improvements in PANSS-positive (r = 0.64, p < 0.01), PANSS negative (rho = 0.51, p = 0.01), and PANSS total (rho = 0.63, p < 0.01) ratings and a negative relationship with change in GAF (r = -0.55, p < 0.01). Clinical response is related to baseline striatal dopaminergic function. Differences in dopaminergic function between responders and non-responders are present at first episode of psychosis, consistent with dopaminergic and non-dopaminergic sub-types in psychosis, and potentially indicating a neurochemical basis to stratify psychosis.
精神病的治疗反应存在差异。确定其背后的神经生物学机制对于精准医学和开发更好的治疗方法至关重要。有人提出,多巴胺能差异是导致反应变化的基础,而在反应者中纹状体多巴胺合成能力(DSC)升高,而非反应者中则没有改变。因此,我们旨在前瞻性队列中,通过嵌套病例对照比较来对此进行测试。40 名志愿者(26 名首发精神病患者和 14 名对照者)在接受抗精神病治疗前接受了 F-DOPA 正电子发射断层扫描以测量 DSC(Ki)。在基线时以及接受抗精神病治疗至少 4 周后进行临床评估(阳性和阴性综合征量表,PANSS 和总体功能评估,GAF)。以 PANSS 总分改善>50%定义为反应。患者至少随访 6 个月,并应用缓解标准。关联纹状体中的 Ki 存在显著的组间效应(F=7.9,p=0.001)。与非反应者(Cohen's d=1.55,p=0.01)和对照组(Cohen's d=1.31,p=0.02)相比,反应者的 Ki 明显更高。Ki 与 PANSS 阳性评分(r=0.64,p<0.01)、PANSS 阴性评分(rho=0.51,p=0.01)和 PANSS 总分(rho=0.63,p<0.01)的改善呈显著正相关,与 GAF 变化呈负相关(r=-0.55,p<0.01)。临床反应与基线纹状体多巴胺能功能有关。在精神病首次发作时,反应者和非反应者之间的多巴胺能功能差异就已经存在,这与精神病中的多巴胺能和非多巴胺能亚型一致,并且可能表明精神分裂症具有神经化学基础进行分层。