Ansari Ishtyaque, Ansari Ashfaque, Graison Arjun Antony, Patil Anuradha J, Joshi Hitendra
Department of Neurosurgery, MGM Medical College & Hospital, Aurangabad, India.
Department of ENT, MGM Medical College & Hospital, Aurangabad, India.
Case Rep Otolaryngol. 2018 Mar 4;2018:4074905. doi: 10.1155/2018/4074905. eCollection 2018.
Schwannomas, also known as neurilemmomas, are benign peripheral nerve sheath tumors. They originate from any nerve covered with schwann cell sheath. Schwannomas constitute 25-45% of tumors of the head and neck. About 4% of head and neck schwannomas present as a sinonasal schwannoma. Brachial plexus schwannoma constitute only about 5% of schwannomas. Cervical vagal schwannomas constitute about 2-5% of neurogenic tumors.
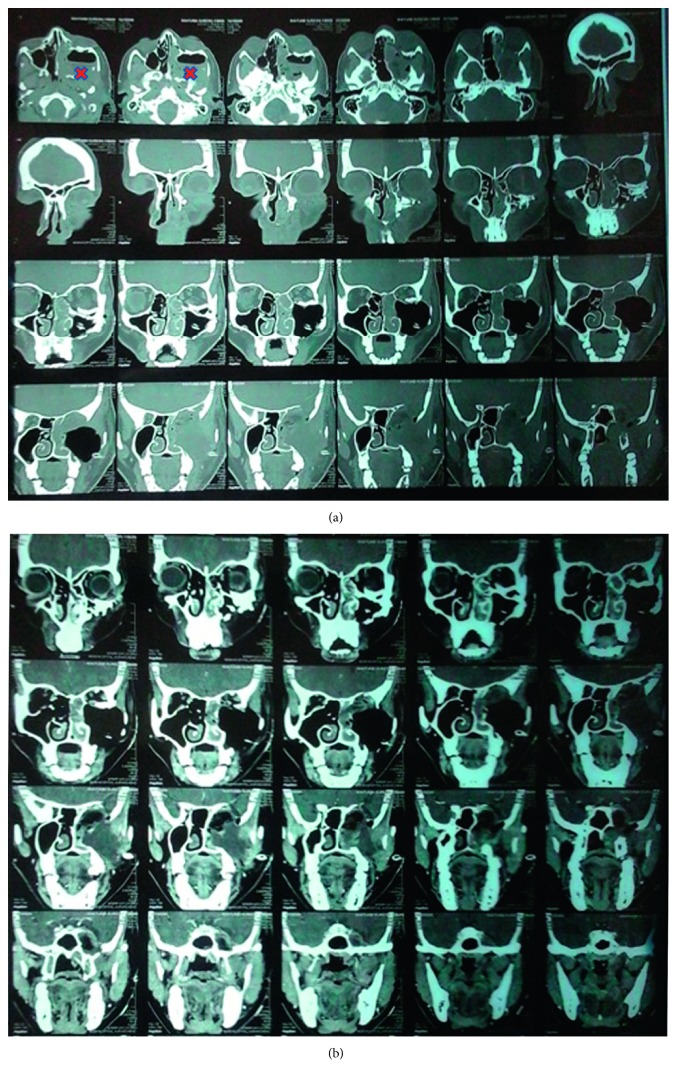
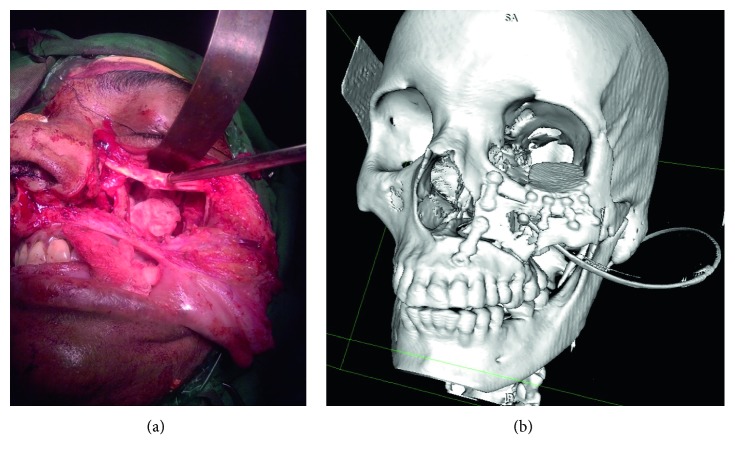
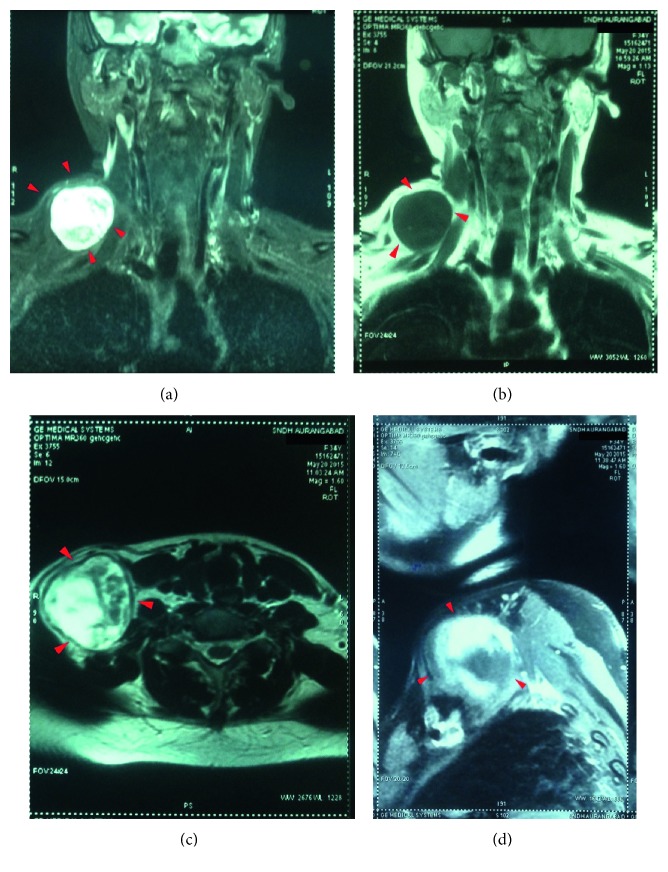
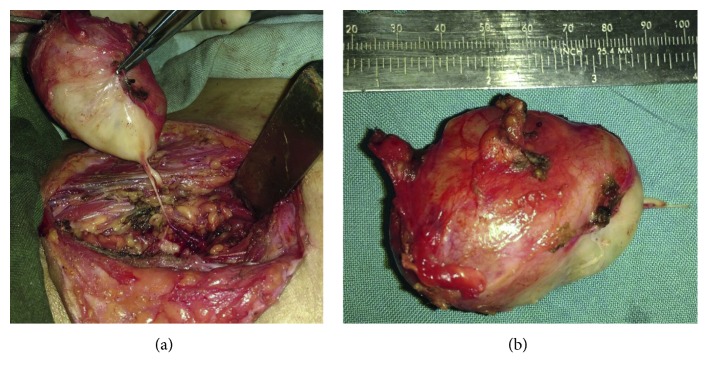
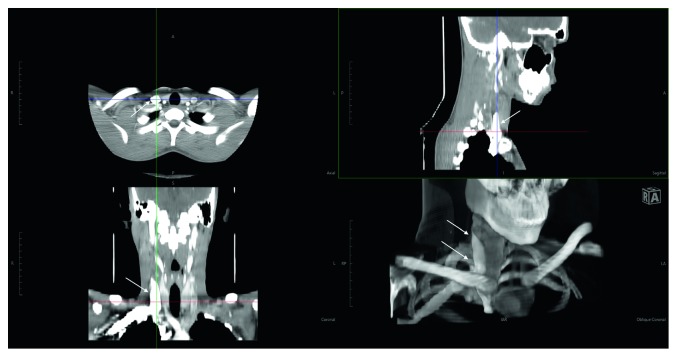
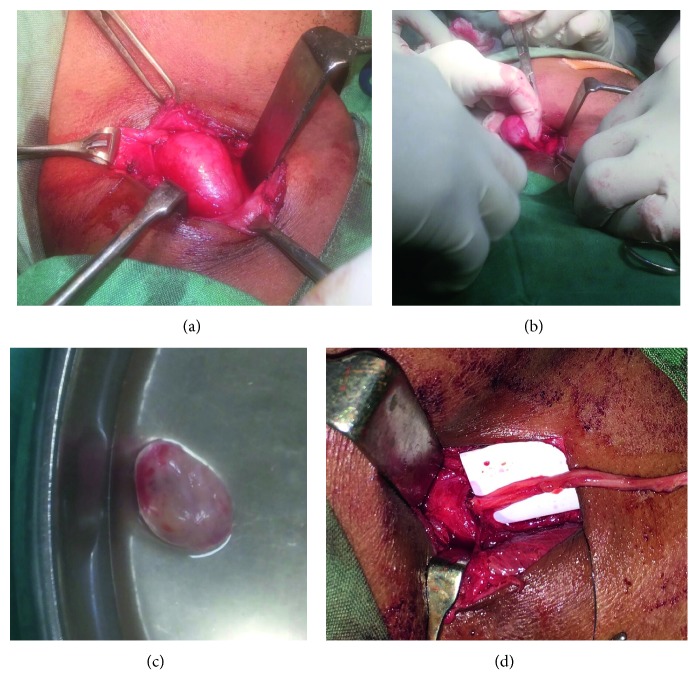
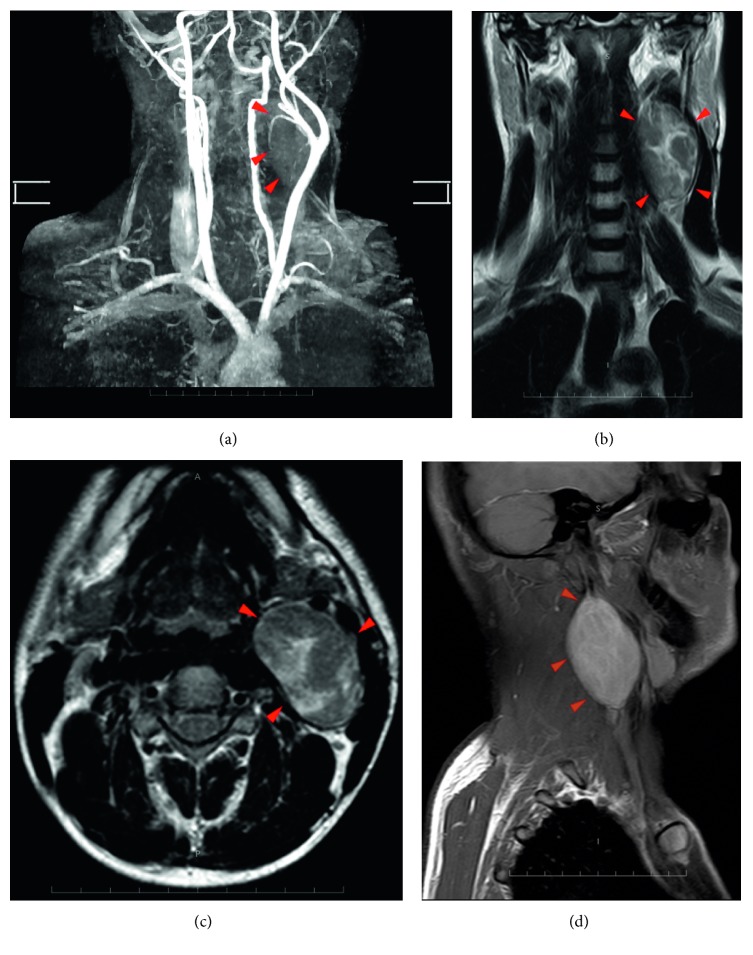
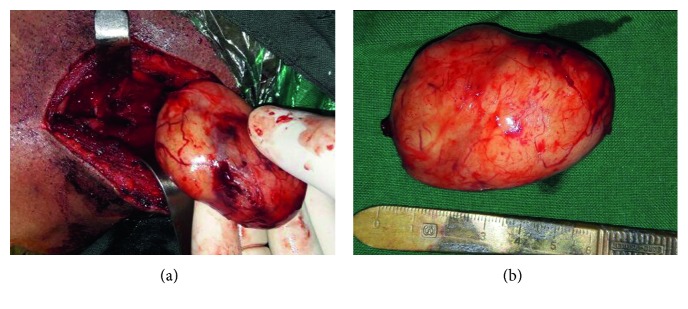
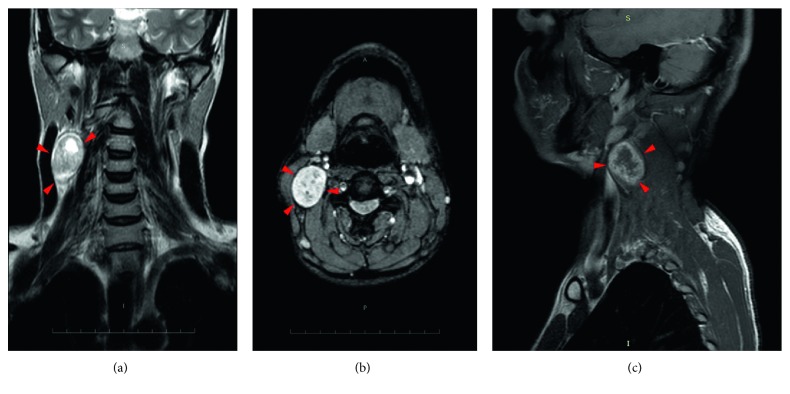
We present a case series of 5 patients of schwannomas, one arising from the maxillary branch of trigeminal nerve in the maxillary sinus, second arising from the brachial plexus, third arising from the cervical vagus, and two arising from cervical spinal nerves.
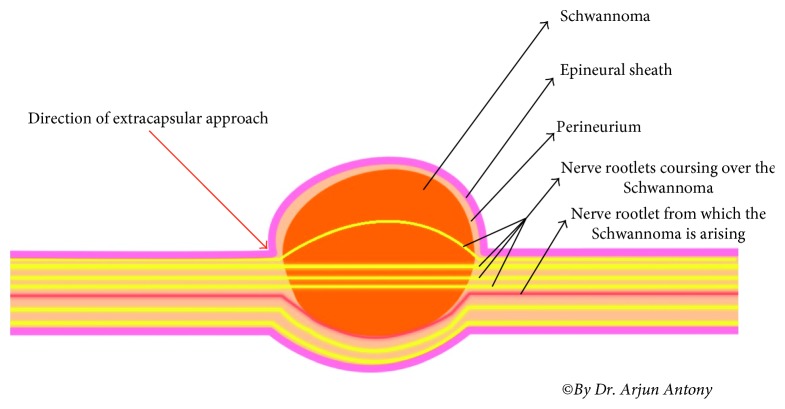
Complete extracapsular excision of the tumors was achieved by microneurosurgical technique with preservation of nerve of origin in all except one.
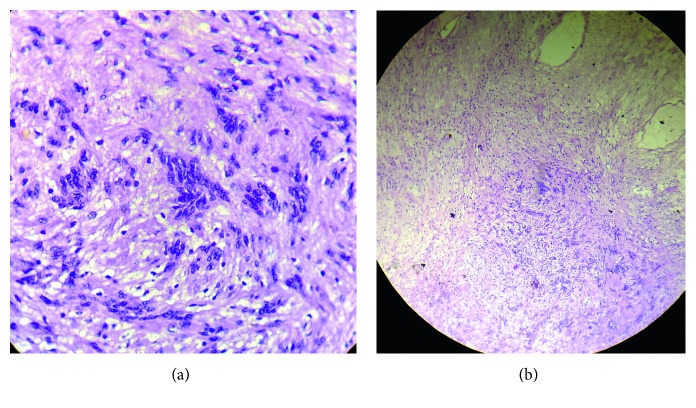
Head and neck schwannoma though rare should be considered as a differential diagnosis of a unilateral slow growing mass in the head and neck region, particularly in an adult. Schwannomas are always a diagnostic dilemma as they are asymptomatic for long time, and histopathology is the gold standard for diagnosis. As a rule, treatment is surgical and dictated by the location of the tumor and nerve of origin. Due to its rarity, complex anatomical location and morbidity risk postexcision, they can pose a formidable challenge to surgeons. This study aims to describe the presentation, workup, surgical technique, and outcome.
施万细胞瘤,也称为神经鞘瘤,是一种良性周围神经鞘膜肿瘤。它们起源于任何被施万细胞鞘覆盖的神经。施万细胞瘤占头颈部肿瘤的25% - 45%。约4%的头颈部施万细胞瘤表现为鼻窦施万细胞瘤。臂丛神经施万细胞瘤仅占施万细胞瘤的约5%。颈迷走神经施万细胞瘤约占神经源性肿瘤的2% - 5%。
我们报告了一组5例施万细胞瘤病例,1例起源于上颌窦内的三叉神经上颌支,第2例起源于臂丛神经,第3例起源于颈迷走神经,另外2例起源于颈脊神经。
通过显微神经外科技术实现了肿瘤的完整包膜外切除,除1例患者外,其余患者均保留了起源神经。
头颈部施万细胞瘤虽然罕见,但应被视为头颈部单侧缓慢生长肿块的鉴别诊断之一,尤其是在成年人中。施万细胞瘤由于长期无症状,一直是诊断难题,组织病理学是诊断的金标准。通常,治疗方法为手术,具体取决于肿瘤的位置和起源神经。由于其罕见性、复杂的解剖位置以及切除后的发病风险,它们对外科医生构成了巨大挑战。本研究旨在描述其临床表现、检查、手术技术及结果。