Gregor James C, Williamson Martin, Dajnowiec Dorota, Sattin Bernie, Sabot Erik, Salh Baljinder
Division of Gastroenterology, Department of Medicine, Western University, London, ON, Canada.
Janssen Inc., Toronto, ON, Canada.
Patient Prefer Adherence. 2018 Apr 10;12:505-513. doi: 10.2147/PPA.S152872. eCollection 2018.
Given the large armamentarium of therapies for inflammatory bowel disease (IBD), physicians cannot fully describe all treatments to patients and, therefore, make assumptions regarding treatment attributes communicated to patients. This study aimed to assess out-of-pocket willingness-to-pay that IBD patients allocate to treatment attributes.
Adult patients receiving therapy for IBD were invited to access a cross-sectional web-based discrete-choice experiment (May 22-August 31, 2015) that presented paired medication scenarios with varying efficacy, safety, and administration parameters. Preference weights and willingness-to-pay for each attribute level were assessed by a hierarchical Bayes method including a multinomial logit model.
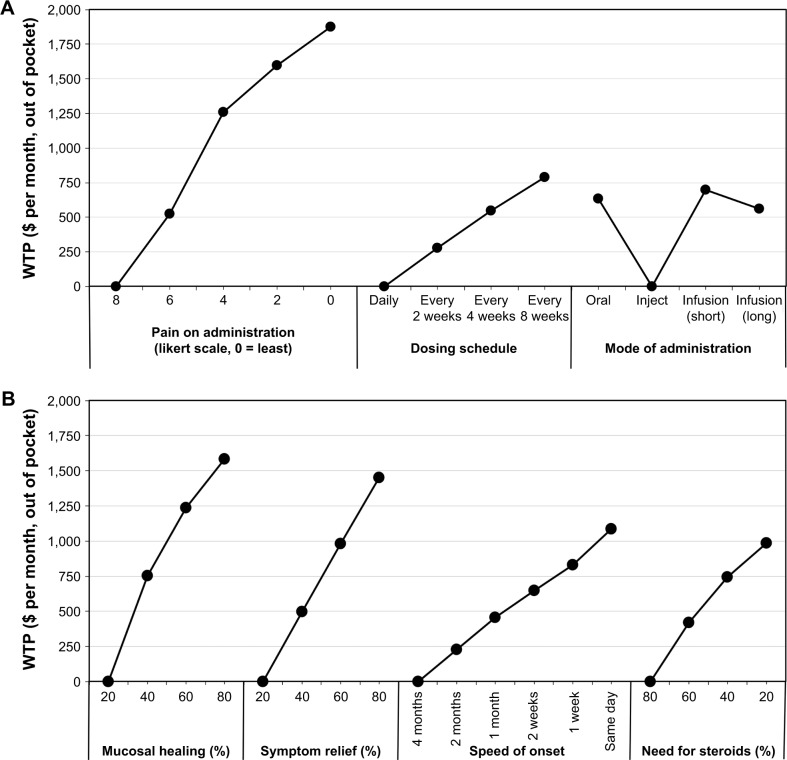
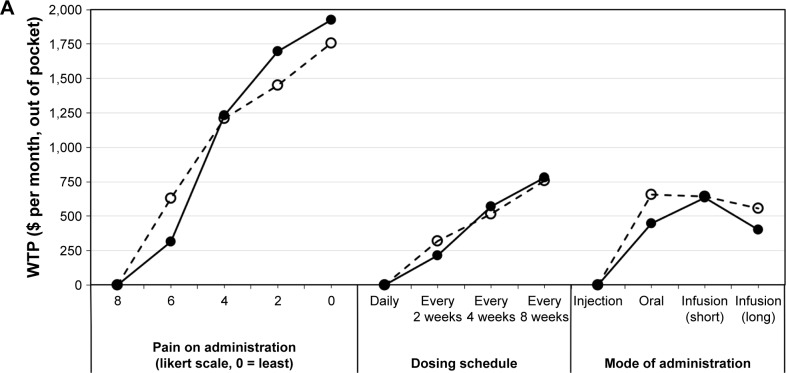
A total of 586 IBD patients were included, 404 (68.9%) with Crohn's disease and 182 (31.1%) with ulcerative colitis. Genders were evenly distributed; the majority of patients (70.1%) were 50 years or younger and had postsecondary education (75.4%), while the median health status was 7 (Likert scale: 1 [poor] - 10 [perfect]). Regarding relative preference-weight estimates, for the average respondent, reducing pain during administration, mucosal healing, and symptom relief were the highest-ranking attributes. Conversely, infusion reactions and risk of hospitalization or surgery were the lowest-ranking attributes. In multivariate analysis, patient sociodemographics did not affect the rank order of attributes although small differences were observed between asymptomatic and symptomatic patients in the previous year.
This study has important implications related to understanding patient preferences and designing patient-centered strategies. IBD patients prioritize treatments with low administration pain. Additionally, these results concur with treatment guidelines emphasizing patients' preference for mucosal healing and symptom control.
鉴于治疗炎症性肠病(IBD)的疗法种类繁多,医生无法向患者全面描述所有治疗方法,因此,他们会对向患者传达的治疗属性进行假设。本研究旨在评估IBD患者为治疗属性支付的自付意愿。
邀请接受IBD治疗的成年患者参与一项基于网络的横断面离散选择实验(2015年5月22日至8月31日),该实验呈现了具有不同疗效、安全性和给药参数的成对药物场景。通过包括多项逻辑回归模型的分层贝叶斯方法评估每个属性水平的偏好权重和支付意愿。
共纳入586例IBD患者,其中404例(68.9%)患有克罗恩病,182例(31.1%)患有溃疡性结肠炎。性别分布均匀;大多数患者(70.1%)年龄在50岁及以下,接受过高等教育(75.4%),而健康状况中位数为7(李克特量表:1[差]-10[完美])。关于相对偏好权重估计,对于一般受访者而言,减轻给药期间的疼痛、黏膜愈合和症状缓解是排名最高的属性。相反,输液反应以及住院或手术风险是排名最低的属性。在多变量分析中,患者的社会人口统计学特征并未影响属性的排名顺序,尽管在前一年无症状和有症状患者之间观察到了细微差异。
本研究对于理解患者偏好和设计以患者为中心的策略具有重要意义。IBD患者优先选择给药疼痛低的治疗方法。此外,这些结果与强调患者对黏膜愈合和症状控制偏好的治疗指南一致。