From the Departments of Epidemiology (K.R., G.R.S., P.L.W., S.H.-D., K.P.) and Biostatistics (P.L.W., D.E.S.) and the Center for Biostatistics and AIDS Research (Y.H., D.E.S., K.P.), Harvard T.H. Chan School of Public Health, and the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School (K.R.), Boston; the Department of Pediatrics, Northwestern University Feinberg School of Medicine, Chicago (E.G.C.); the Department of Medicine and Division of Infectious Diseases, David Geffen School of Medicine at the University of California, Los Angeles, Los Angeles (J.S.C., R.M.H.); and the Department of Pediatrics, University of Colorado School of Medicine, Aurora (E.B.).
N Engl J Med. 2018 Apr 26;378(17):1593-1603. doi: 10.1056/NEJMoa1701666.
In a previous trial of antiretroviral therapy (ART) involving pregnant women with human immunodeficiency virus (HIV) infection, those randomly assigned to receive tenofovir, emtricitabine, and ritonavir-boosted lopinavir (TDF-FTC-LPV/r) had infants at greater risk for very premature birth and death within 14 days after delivery than those assigned to receive zidovudine, lamivudine, and ritonavir-boosted lopinavir (ZDV-3TC-LPV/r).
Using data from two U.S.-based cohort studies, we compared the risk of adverse birth outcomes among infants with in utero exposure to ZDV-3TC-LPV/r, TDF-FTC-LPV/r, or TDF-FTC with ritonavir-boosted atazanavir (ATV/r). We evaluated the risk of preterm birth (<37 completed weeks of gestation), very preterm birth (<34 completed weeks), low birth weight (<2500 g), and very low birth weight (<1500 g). Risk ratios with 95% confidence intervals were estimated with the use of modified Poisson models to adjust for confounding.
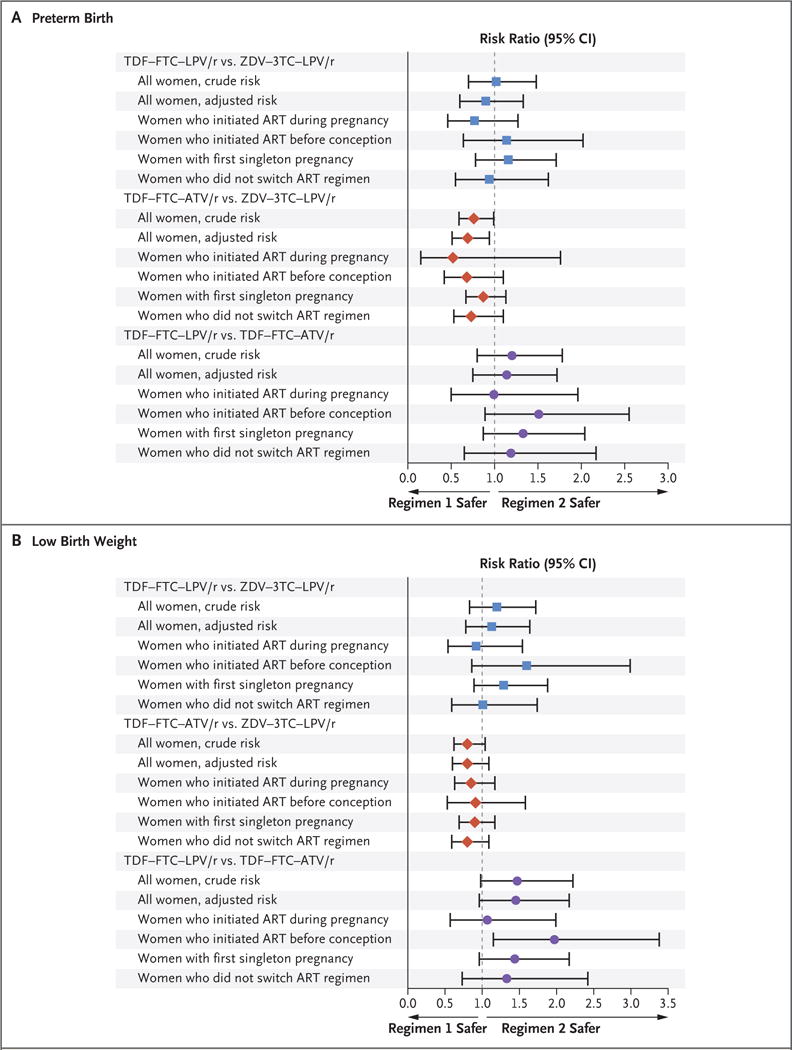
There were 4646 birth outcomes. Few infants or fetuses were exposed to TDF-FTC-LPV/r (128 [2.8%]) as the initial ART regimen during gestation, in contrast with TDF-FTC-ATV/r (539 [11.6%]) and ZDV-3TC-LPV/r (954 [20.5%]). As compared with women receiving ZDV-3TC-LPV/r, women receiving TDF-FTC-LPV/r had a similar risk of preterm birth (risk ratio, 0.90; 95% confidence interval [CI], 0.60 to 1.33) and low birth weight (risk ratio, 1.13; 95% CI, 0.78 to 1.64). As compared to women receiving TDF-FTC-ATV/r, women receiving TDF-FTC-LPV/r had a similar or slightly higher risk of preterm birth (risk ratio, 1.14; 95% CI, 0.75 to 1.72) and low birth weight (risk ratio, 1.45; 95% CI, 0.96 to 2.17). There were no significant differences between regimens in the risk of very preterm birth or very low birth weight.
The risk of adverse birth outcomes was not higher with TDF-FTC-LPV/r than with ZDV-3TC-LPV/r or TDF-FTC-ATV/r among HIV-infected women and their infants in the United States, although power was limited for some comparisons. (Funded by the National Institutes of Health and others.).
在一项针对人类免疫缺陷病毒(HIV)感染孕妇的抗逆转录病毒治疗(ART)的先前试验中,与接受齐多夫定、拉米夫定和利托那韦增强洛匹那韦(ZDV-3TC-LPV/r)治疗的随机分组相比,接受替诺福韦、恩曲他滨和利托那韦增强洛匹那韦(TDF-FTC-LPV/r)治疗的孕妇所生婴儿在出生后 14 天内极早产和死亡的风险更高。
我们利用两项美国队列研究的数据,比较了宫内暴露于 ZDV-3TC-LPV/r、TDF-FTC-LPV/r 或 TDF-FTC 联合利托那韦增强的阿扎那韦(ATV/r)的婴儿发生不良出生结局的风险。我们评估了早产(<37 周妊娠)、极早产(<34 周妊娠)、低出生体重(<2500g)和极低出生体重(<1500g)的风险。使用修正泊松模型评估风险比(RR)和 95%置信区间(CI),以调整混杂因素。
共有 4646 例出生结局。与 TDF-FTC-ATV/r(539[11.6%])和 ZDV-3TC-LPV/r(954[20.5%])相比,作为妊娠期初始 ART 方案,接受 TDF-FTC-LPV/r 的婴儿或胎儿很少(128[2.8%])。与接受 ZDV-3TC-LPV/r 的妇女相比,接受 TDF-FTC-LPV/r 的妇女早产的风险相似(RR,0.90;95%CI,0.60 至 1.33)和低出生体重(RR,1.13;95%CI,0.78 至 1.64)。与接受 TDF-FTC-ATV/r 的妇女相比,接受 TDF-FTC-LPV/r 的妇女早产的风险相似或略高(RR,1.14;95%CI,0.75 至 1.72)和低出生体重(RR,1.45;95%CI,0.96 至 2.17)。不同方案之间极早产或极低出生体重的风险无显著差异。
在美国感染 HIV 的妇女及其婴儿中,与 ZDV-3TC-LPV/r 或 TDF-FTC-ATV/r 相比,TDF-FTC-LPV/r 并未增加不良出生结局的风险,尽管某些比较的效力有限。(由美国国立卫生研究院和其他机构资助)。