Department of Hematology, Karolinska University Hospital Huddinge, Stockholm, Sweden.
Department of Hematology, Instituto de Biomedicina de Sevilla (IBIS), Hospital Universitario Virgen del Rocío/CSIC/Universidad de Sevilla, Seville, Spain.
Med Oncol. 2018 Apr 25;35(6):79. doi: 10.1007/s12032-018-1127-2.
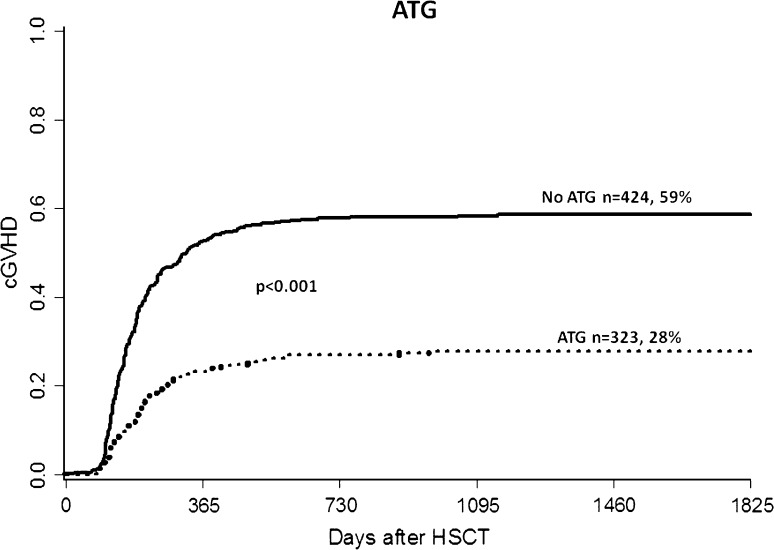
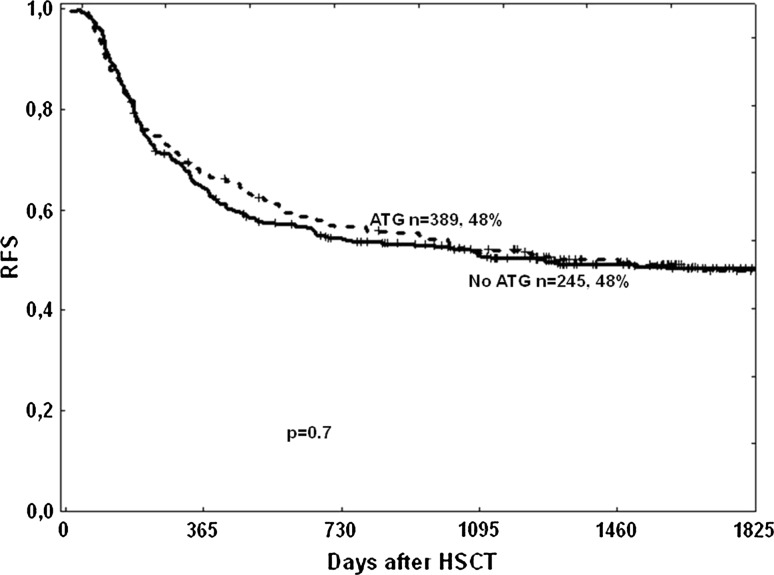
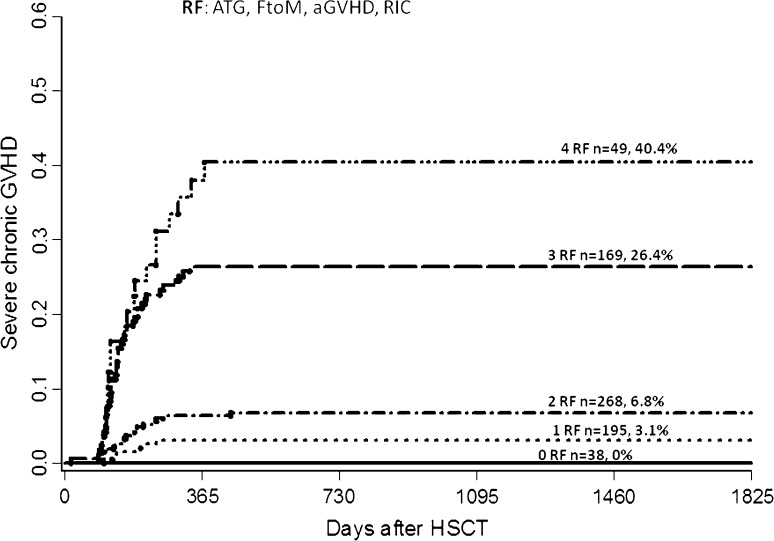
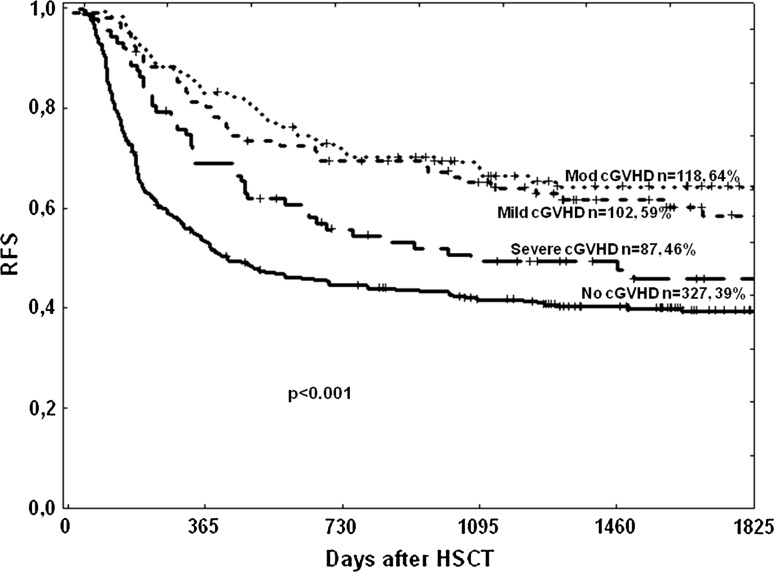
Chronic graft-versus-host disease (cGVHD) remains a major cause of morbidity and mortality after allogeneic hematopoietic stem cell transplantation (HSCT). Aim is to identify risk factors for the development of cGVHD in a multicenter setting. Patients transplanted between 2000 and 2006 were analyzed (n = 820). Donors were HLA-identical siblings (57%), matched unrelated donors (30%), and HLA-A, B or DR antigen mismatched (13%). Reduced intensity conditioning (RIC) was given to 65% of patients. Overall incidence of cGVHD was 46% for patients surviving more than 100 days after HSCT (n = 747). Older patient age [HR 1.15, p < 0.001], prior acute GVHD [1.30, p = 0.024], and RIC [1.36, p = 0.028] increased overall cGVHD. In addition, RIC [4.85, p < 0.001], prior aGVHD [2.14, p = 0.001] and female donor to male recipient [1.80, p = 0.008] increased the risk of severe cGVHD. ATG had a protective effect for both overall [0.41, p < 0.001] and severe cGVHD [0.20, p < 0.001]. Relapse-free survival (RFS) was impaired in patients with severe cGVHD. RIC, prior aGVHD, and female-to-male donation increase the risk of severe cGVHD. ATG reduces the risk of all grades of cGVHD without hampering RFS. GVHD prophylaxis may be tailored according to the risk profile of patients.
慢性移植物抗宿主病(cGVHD)仍然是异基因造血干细胞移植(HSCT)后发病率和死亡率的主要原因。目的是在多中心环境中确定 cGVHD 发展的危险因素。分析了 2000 年至 2006 年间移植的患者(n=820)。供体为 HLA 完全匹配的同胞(57%)、匹配的无关供体(30%)和 HLA-A、B 或 DR 抗原错配(13%)。65%的患者接受了强度降低的调理。HSCT 后 100 天以上存活的患者中 cGVHD 的总体发生率为 46%(n=747)。患者年龄较大[HR 1.15,p<0.001]、急性移植物抗宿主病(GVHD)既往史[1.30,p=0.024]和强度降低的调理[1.36,p=0.028]均增加了整体 cGVHD 的发生率。此外,强度降低的调理[4.85,p<0.001]、急性 GVHD 既往史[2.14,p=0.001]和女性供体至男性受体[1.80,p=0.008]增加了严重 cGVHD 的风险。ATG 对整体[0.41,p<0.001]和严重 cGVHD [0.20,p<0.001]均具有保护作用。有严重 cGVHD 的患者无复发生存率(RFS)受损。严重 cGVHD 患者的 RIC、急性 GVHD 既往史和女性供体至男性受体增加了风险。ATG 降低了所有等级 cGVHD 的风险,而不会影响 RFS。根据患者的风险状况,可以调整 GVHD 的预防措施。