Ro Hyung-Suk, Shin Jin Yong, Sabbagh Mohamed Diya, Roh Si-Gyun, Chang Suk Choo, Lee Nae-Ho
Department of Plastic and Reconstructive Surgery, Medical School of Chonbuk National University.
Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Republic of Korea.
Medicine (Baltimore). 2018 Apr;97(17):e0563. doi: 10.1097/MD.0000000000010563.
Health care providers commonly encounter blisters when treating burn patients. The question as to whether burn blisters should be drained or deroofed has long been debated. To our knowledge, there has been no controlled, randomized clinical trial to determine which treatment is the best management option.
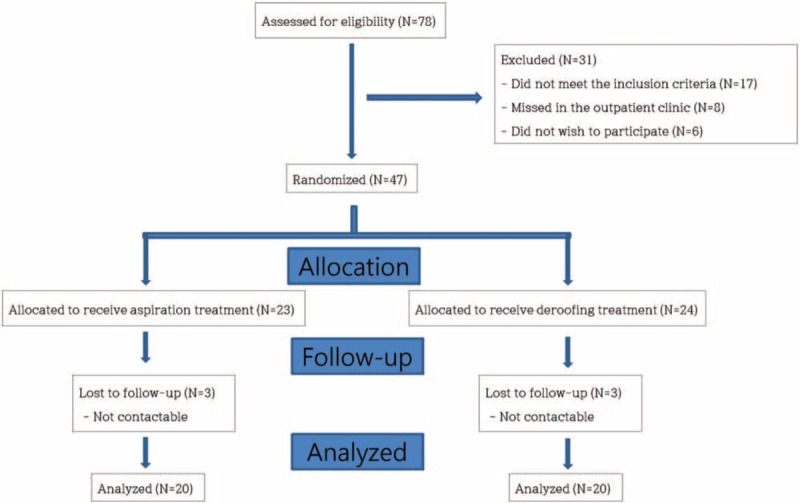
Between March 2016, and September 2016; 40 patients with burn blisters greater than 6-mm were enrolled in our study. Patients were randomized into 2 groups: aspiration group and deroofing group. The number of days to complete re-epithelialization was noted. Patient and Observer Scar Assessment Scale data were recorded from subjects and investigators at 4 time points. Pain during dressing changes was evaluated using a visual pain scale. Bacterial cultures were also obtained.
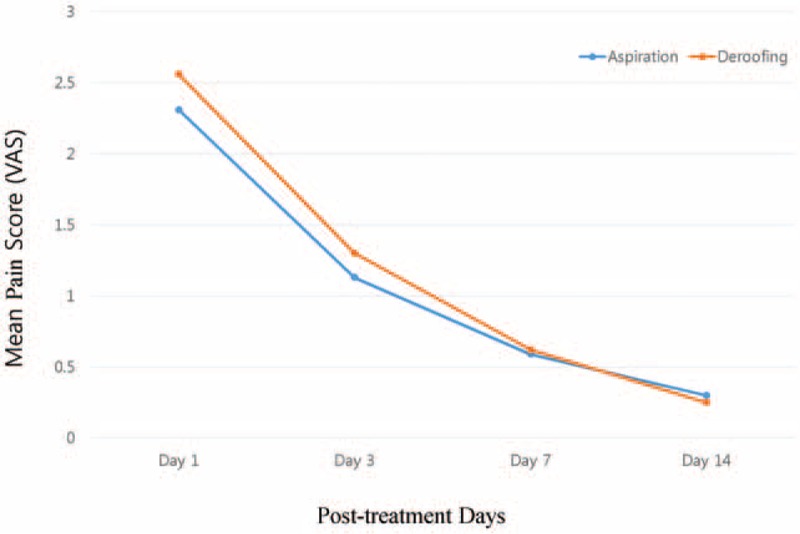
Average number of days to complete wound healing was 12 days in the aspiration group and 12.55 days in deroofing group. On the Patient and Observer Scar Assessment Scale, investigators found that the aspiration group scars demonstrated improvements in relief and thickness while subjects rated aspiration scars better in terms of pain. Patients with palm/sole blister in the deroofing group scored higher than aspiration group on the visual analogue pain score but it was also not statistically significant (2.66 vs 3.25). The overall incidence of colonization with microorganisms in each group was not significant (15% vs 40%).
Neither aspiration nor deroofing is a superior treatment of burn blister. However, some objective indicators suggest that aspiration treatment might be more effective than deroofing treatment.
医疗保健人员在治疗烧伤患者时经常会遇到水泡。关于烧伤水泡是否应该引流或去除疱皮的问题长期以来一直存在争议。据我们所知,尚无对照的随机临床试验来确定哪种治疗是最佳的管理选择。
在2016年3月至2016年9月期间,40例烧伤水泡大于6毫米的患者纳入我们的研究。患者被随机分为两组:抽吸组和去除疱皮组。记录完成再上皮化的天数。在4个时间点从受试者和研究者处记录患者和观察者瘢痕评估量表数据。使用视觉疼痛量表评估换药时的疼痛。还进行了细菌培养。
抽吸组完成伤口愈合的平均天数为12天,去除疱皮组为12.55天。在患者和观察者瘢痕评估量表上,研究者发现抽吸组的瘢痕在缓解和厚度方面有改善,而受试者认为抽吸瘢痕在疼痛方面更好。去除疱皮组手掌/足底水泡患者的视觉模拟疼痛评分高于抽吸组,但也无统计学意义(2.66对3.25)。每组微生物定植的总体发生率无显著差异(15%对40%)。
抽吸和去除疱皮都不是烧伤水泡的优越治疗方法。然而,一些客观指标表明抽吸治疗可能比去除疱皮治疗更有效。