Department of Geriatric Medicine, Lyon Teaching Hospital, Lyon, France.
The Nuffield Trust, London, UK.
Lancet. 2018 May 5;391(10132):1775-1782. doi: 10.1016/S0140-6736(18)30668-8. Epub 2018 Apr 26.
Older people are increasing users of health care globally. We aimed to establish whether older people with characteristics of frailty and who are at risk of adverse health-care outcomes could be identified using routinely collected data.
A three-step approach was used to develop and validate a Hospital Frailty Risk Score from International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) diagnostic codes. First, we carried out a cluster analysis to identify a group of older people (≥75 years) admitted to hospital who had high resource use and diagnoses associated with frailty. Second, we created a Hospital Frailty Risk Score based on ICD-10 codes that characterised this group. Third, in separate cohorts, we tested how well the score predicted adverse outcomes and whether it identified similar groups as other frailty tools.
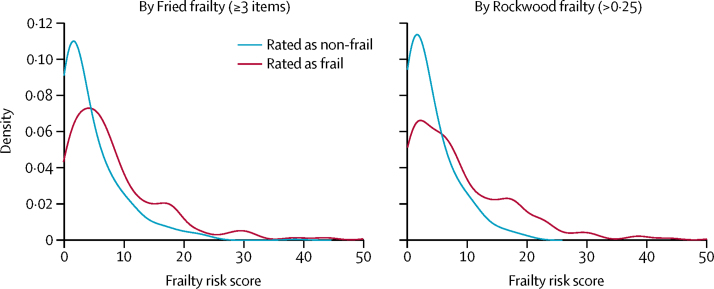
In the development cohort (n=22 139), older people with frailty diagnoses formed a distinct group and had higher non-elective hospital use (33·6 bed-days over 2 years compared with 23·0 bed-days for the group with the next highest number of bed-days). In the national validation cohort (n=1 013 590), compared with the 429 762 (42·4%) patients with the lowest risk scores, the 202 718 (20·0%) patients with the highest Hospital Frailty Risk Scores had increased odds of 30-day mortality (odds ratio 1·71, 95% CI 1·68-1·75), long hospital stay (6·03, 5·92-6·10), and 30-day readmission (1·48, 1·46-1·50). The c statistics (ie, model discrimination) between individuals for these three outcomes were 0·60, 0·68, and 0·56, respectively. The Hospital Frailty Risk Score showed fair overlap with dichotomised Fried and Rockwood scales (kappa scores 0·22, 95% CI 0·15-0·30 and 0·30, 0·22-0·38, respectively) and moderate agreement with the Rockwood Frailty Index (Pearson's correlation coefficient 0·41, 95% CI 0·38-0·47).
The Hospital Frailty Risk Score provides hospitals and health systems with a low-cost, systematic way to screen for frailty and identify a group of patients who are at greater risk of adverse outcomes and for whom a frailty-attuned approach might be useful.
National Institute for Health Research.
老年人在全球范围内越来越多地使用医疗保健。我们旨在确定是否可以使用常规收集的数据来识别具有脆弱特征和可能出现不良医疗保健结果风险的老年人。
采用三步法从国际疾病分类第十版(ICD-10)诊断代码中建立和验证医院脆弱性风险评分。首先,我们进行聚类分析以确定一组资源利用高且与脆弱性相关的诊断的老年(≥75 岁)住院患者。其次,我们基于描述该组的 ICD-10 代码创建了医院脆弱性风险评分。第三,在单独的队列中,我们测试了该评分预测不良结局的效果,以及它是否与其他脆弱性工具一样可以识别出相似的人群。
在发展队列(n=22139)中,具有脆弱性诊断的老年人形成了一个独特的群体,非选择性住院使用更高(2 年中 33.6 个床位天,而床位天数第二高的群体为 23.0 个床位天)。在全国验证队列(n=1013590)中,与风险评分最低的 429762(42.4%)名患者相比,风险评分最高的 202718(20.0%)名患者在 30 天内死亡的可能性更高(比值比 1.71,95%CI 1.68-1.75)、住院时间更长(6.03,5.92-6.10)和 30 天内再入院(1.48,1.46-1.50)。这三个结局的个体之间的 C 统计量(即模型区分度)分别为 0.60、0.68 和 0.56。医院脆弱性风险评分与二分法 Fried 和 Rockwood 量表显示出适度的重叠(kappa 评分分别为 0.22、95%CI 0.15-0.30 和 0.30、0.22-0.38),与 Rockwood 脆弱性指数的一致性适中(Pearson 相关系数为 0.41,95%CI 0.38-0.47)。
医院脆弱性风险评分可为医院和卫生系统提供一种低成本、系统的方法来筛查脆弱性,并确定一组更容易出现不良结局的患者,这些患者可能需要进行脆弱性调整的方法。
英国国家健康研究所。