Le Pogam Marie-Annick, Seematter-Bagnoud Laurence, Niemi Tapio, Assouline Dan, Gross Nathan, Trächsel Bastien, Rousson Valentin, Peytremann-Bridevaux Isabelle, Burnand Bernard, Santos-Eggimann Brigitte
Department of Epidemiology and Health Systems, Centre for Primary Care and Public Health (Unisanté), University of Lausanne, 10 Route de la Corniche, Lausanne 1010, Switzerland.
Department of Training, Research and Innovation, Centre for Primary Care and Public Health (Unisanté), University of Lausanne, 113 Route de Berne, Lausanne 1010, Switzerland.
EClinicalMedicine. 2022 Jan 10;44:101260. doi: 10.1016/j.eclinm.2021.101260. eCollection 2022 Feb.
Most claims-based frailty instruments have been designed for group stratification of older populations according to the risk of adverse health outcomes and not frailty itself. We aimed to develop and validate a tool based on one-year hospital discharge data for stratification on Fried's frailty phenotype (FP).
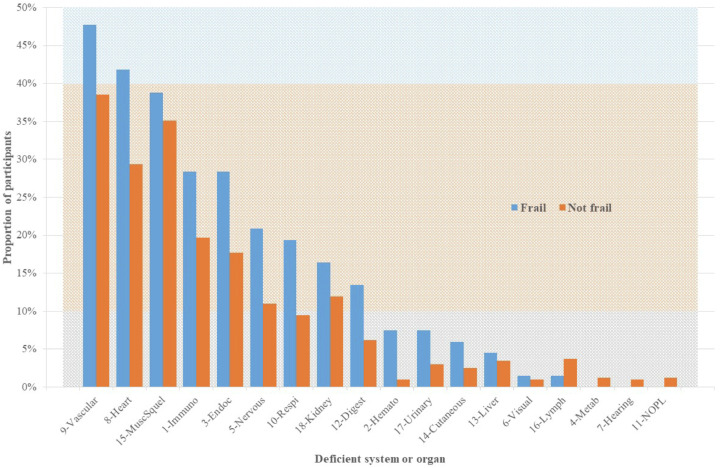
We used a three-stage development/validation approach. First, we created a clinical knowledge-driven electronic frailty score (eFS) calculated as the number of deficient organs/systems among 18 critical ones identified from the (ICD-10) diagnoses coded in the year before FP assessment. Second, for eFS development and internal validation, we linked individual records from the Lc65+ cohort database to inpatient discharge data from Lausanne University Hospital (CHUV) for the period 2004-2015. The development/internal validation sample included community-dwelling, non-institutionalised residents of Lausanne (Switzerland) recruited in the Lc65+ cohort in three waves (2004, 2009, and 2014), aged 65-70 years at enrolment, and hospitalised at the CHUV at least once in the year preceding the FP assessment. Using this sample, we selected the best performing model for predicting the dichotomised FP, with the eFS or ICD-10-based variables as predictors. Third, we conducted an external validation using 2016 Swiss nationwide hospital discharge data and compared the performance of the eFS model in predicting 13 adverse outcomes to three models relying on well-designed and validated claims-based scores (Claims-based Frailty Index, Hospital Frailty Risk Score, Dr Foster Global Frailty Score).
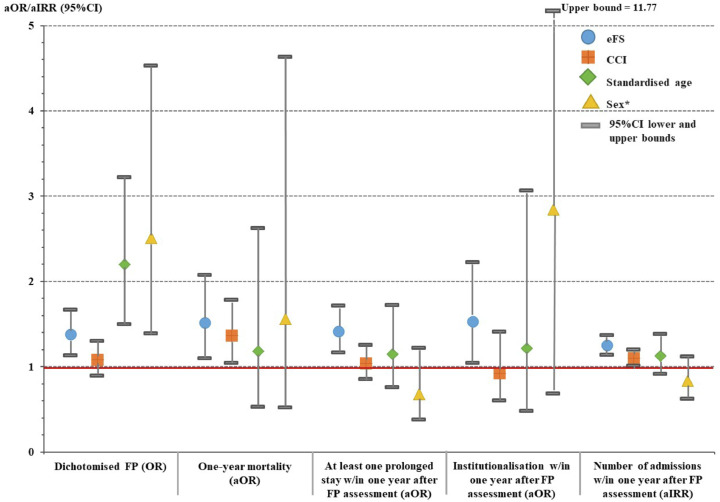
In the development/internal validation sample ( = 469), 14·3% of participants ( 67) were frail. Among 34 models tested, the best-subsets logistic regression model with four predictors (age and sex at FP assessment, time since last hospital discharge, eFS) performed best in predicting the dichotomised FP (area under the curve=0·71; F1 score=0·39) and one-year adverse health outcomes. On the external validation sample ( 54,815; 153 acute care hospitals), the eFS model demonstrated a similar performance to the three other claims-based scoring models. According to the eFS model, the external validation sample showed an estimated prevalence of 56·8% ( 31,135) of frail older inpatients at admission.
The eFS model is an inexpensive, transportable and valid tool allowing reliable group stratification and individual prioritisation for comprehensive frailty assessment and may be applied to both hospitalised and community-dwelling older adults.
The study received no external funding.
大多数基于索赔的衰弱评估工具是为根据不良健康结局风险而非衰弱本身对老年人群进行分组分层而设计的。我们旨在开发并验证一种基于一年期医院出院数据对弗里德衰弱表型(FP)进行分层的工具。
我们采用了三阶段的开发/验证方法。首先,我们创建了一个基于临床知识的电子衰弱评分(eFS),计算方法是在FP评估前一年编码的国际疾病分类第十版(ICD - 10)诊断中确定的18个关键器官/系统中存在缺陷的器官/系统数量。其次,为了进行eFS开发和内部验证,我们将来自Lc65 +队列数据库的个体记录与洛桑大学医院(CHUV)2004 - 2015年期间的住院出院数据相链接。开发/内部验证样本包括在Lc65 +队列中分三批(2004年、2009年和2014年)招募的瑞士洛桑社区居住、非机构化居民,入组时年龄为65 - 70岁,且在FP评估前一年至少在CHUV住院一次。利用这个样本,我们选择了预测二分法FP的最佳表现模型,并将eFS或基于ICD - 10的变量作为预测因子。第三,我们使用2016年瑞士全国医院出院数据进行外部验证,并将eFS模型预测13种不良结局的表现与依赖精心设计和验证的基于索赔的评分模型(基于索赔的衰弱指数、医院衰弱风险评分、福斯特全球衰弱评分)的三种模型进行比较。
在开发/内部验证样本(n = 469)中,14.3%的参与者(n = 67)衰弱。在测试的34个模型中,具有四个预测因子(FP评估时的年龄和性别、上次出院后的时间、eFS)的最佳子集逻辑回归模型在预测二分法FP(曲线下面积 = 0.71;F1分数 = 0.39)和一年期不良健康结局方面表现最佳。在外部验证样本(n = 54,815;153家急性护理医院)中,eFS模型表现出与其他三种基于索赔的评分模型相似的性能。根据eFS模型,外部验证样本显示入院时衰弱老年住院患者的估计患病率为56.8%(n = 31,135)。
eFS模型是一种廉价、可移植且有效的工具,可用于可靠的分组分层和个体优先级排序,以进行全面的衰弱评估,并且可应用于住院和社区居住的老年人。
该研究未获得外部资金。