Burton Graham J, Jauniaux Eric
Department of Physiology, Development and Neuroscience, Centre for Trophoblast Research, University of Cambridge, Cambridge, United Kingdom.
Faculty of Population Health Sciences, EGA Institute for Women's Health, University College London, London, United Kingdom.
Front Physiol. 2018 Apr 12;9:373. doi: 10.3389/fphys.2018.00373. eCollection 2018.
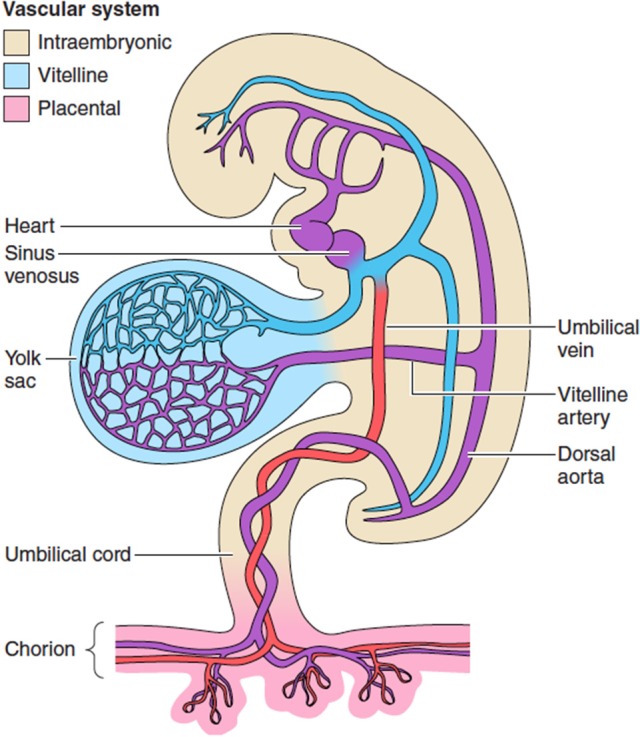
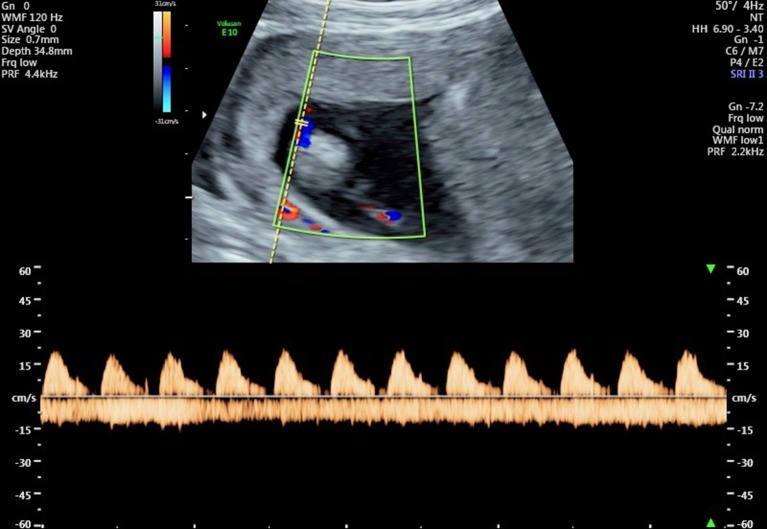
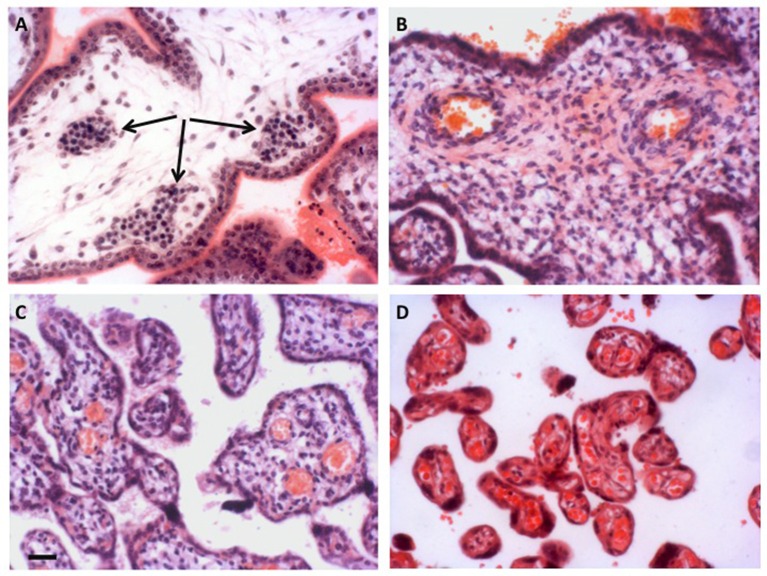
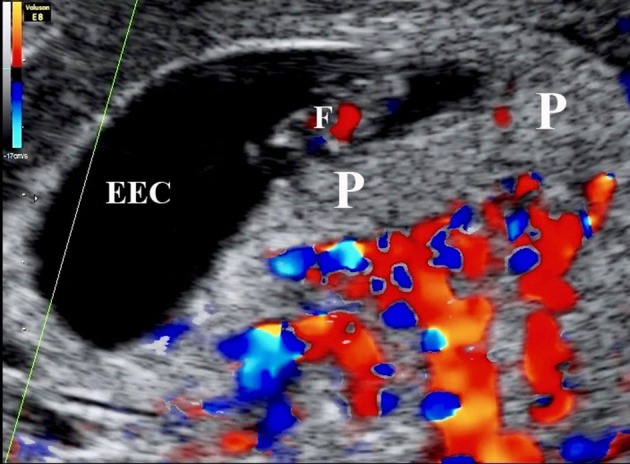
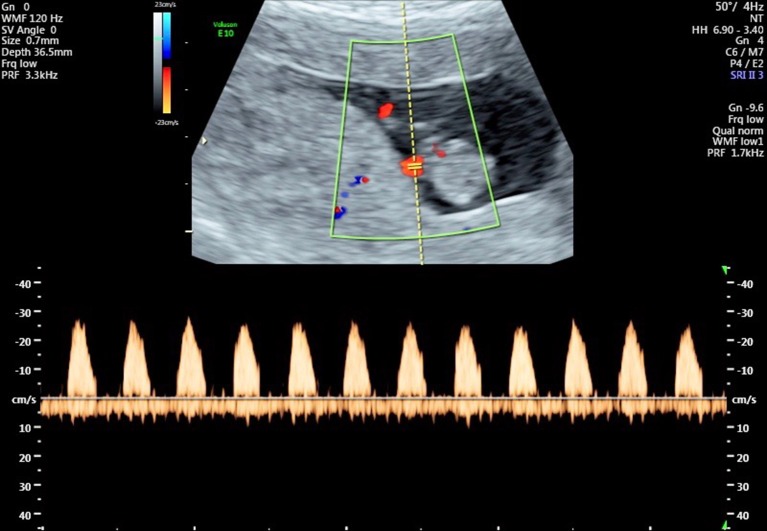
The placenta is the largest fetal organ, and toward the end of pregnancy the umbilical circulation receives at least 40% of the biventricular cardiac output. It is not surprising, therefore, that there are likely to be close haemodynamic links between the development of the placenta and the fetal heart. Development of the placenta is precocious, and in advance of that of the fetus. The placenta undergoes considerable remodeling at the end of the first trimester of pregnancy, and its vasculature is capable of adapting to environmental conditions and to variations in the blood supply received from the mother. There are two components to the placental membranes to consider, the secondary yolk sac and the chorioallantoic placenta. The yolk sac is the first of the extraembryonic membranes to be vascularized, and condensations in the mesenchyme at ~17 days post-conception (p.c.) give rise to endothelial and erythroid precursors. A network of blood vessels is established ~24 days p.c., with the vitelline vein draining through the region of the developing liver into the sinus venosus. Gestational sacs of early pregnancy failures often display aberrant development of the yolk sac, which is likely to be secondary to abnormal fetal development. Vasculogenesis occurs in the villous mesenchyme of the chorioallantoic placenta at a similarly early stage. Nucleated erythrocytes occupy the lumens of the placental capillaries and end-diastolic flow is absent in the umbilical arterial circulation throughout most of the first trimester, indicating a high resistance to blood flow. Resistance begins to fall in the umbilico-placental circulation around 12-14 weeks. During normal early pregnancy the placental capillary network is plastic, and considerable remodeling occurs in response to the local oxygen concentration, and in particular to oxidative stress. In pregnancies complicated by preeclampsia and/or fetal growth restriction, utero-placental malperfusion induces smooth muscle cells surrounding the placental arteries to dedifferentiate and adopt a proliferative phenotype. This change is associated with increased umbilical resistance measured by Doppler ultrasound, and is likely to exert a major effect on the developing heart through the afterload. Thus, both the umbilical and maternal placental circulations may impact on development of the heart.
胎盘是最大的胎儿器官,在妊娠晚期,脐循环至少接受双心室心输出量的40%。因此,胎盘发育与胎儿心脏之间可能存在密切的血流动力学联系也就不足为奇了。胎盘发育早熟,先于胎儿发育。胎盘在妊娠早期三个月末会经历相当大的重塑,其血管系统能够适应环境条件以及来自母体的血液供应变化。胎盘膜有两个组成部分需要考虑,即次级卵黄囊和绒毛膜尿囊胎盘。卵黄囊是第一个血管化的胚外膜,在受精后约17天(p.c.)间充质中的浓缩物产生内皮和红细胞前体。约在受精后24天建立血管网络,卵黄静脉通过发育中的肝脏区域引流到静脉窦。早期妊娠失败的妊娠囊通常显示卵黄囊发育异常,这可能继发于胎儿发育异常。绒毛膜尿囊胎盘的绒毛间充质在相似的早期阶段发生血管生成。有核红细胞占据胎盘毛细血管腔,在妊娠早期的大部分时间里脐动脉循环中舒张末期血流缺失,表明对血流有高阻力。在12 - 14周左右,脐 - 胎盘循环中的阻力开始下降。在正常的早期妊娠期间,胎盘毛细血管网络具有可塑性,会因局部氧浓度,特别是氧化应激而发生相当大的重塑。在子痫前期和/或胎儿生长受限的妊娠中,子宫 - 胎盘灌注不足会诱导胎盘动脉周围的平滑肌细胞去分化并呈现增殖表型。这种变化与通过多普勒超声测量的脐阻力增加有关,并且可能通过后负荷对发育中的心脏产生重大影响。因此,脐循环和母体胎盘循环都可能影响心脏的发育。