Scott Rachel K, Crochet Stacia, Huang Chun-Chih
MedStar Health Research Institute (MHRI), Washington, DC, USA.
MedStar Washington Hospital Center (MWHC), Division of Women's and Infants' Services, Washington, DC, USA.
Infect Dis Obstet Gynecol. 2018 Mar 14;2018:6024698. doi: 10.1155/2018/6024698. eCollection 2018.
To determine the cost-effectiveness of universal maternal HIV screening at time of delivery to decrease mother-to-child transmission (MTCT), by comparing the cost and quality-adjusted life years (QALYs) of universal rapid HIV screening at time of delivery to two current standards of care for prenatal HIV screening in the United States.
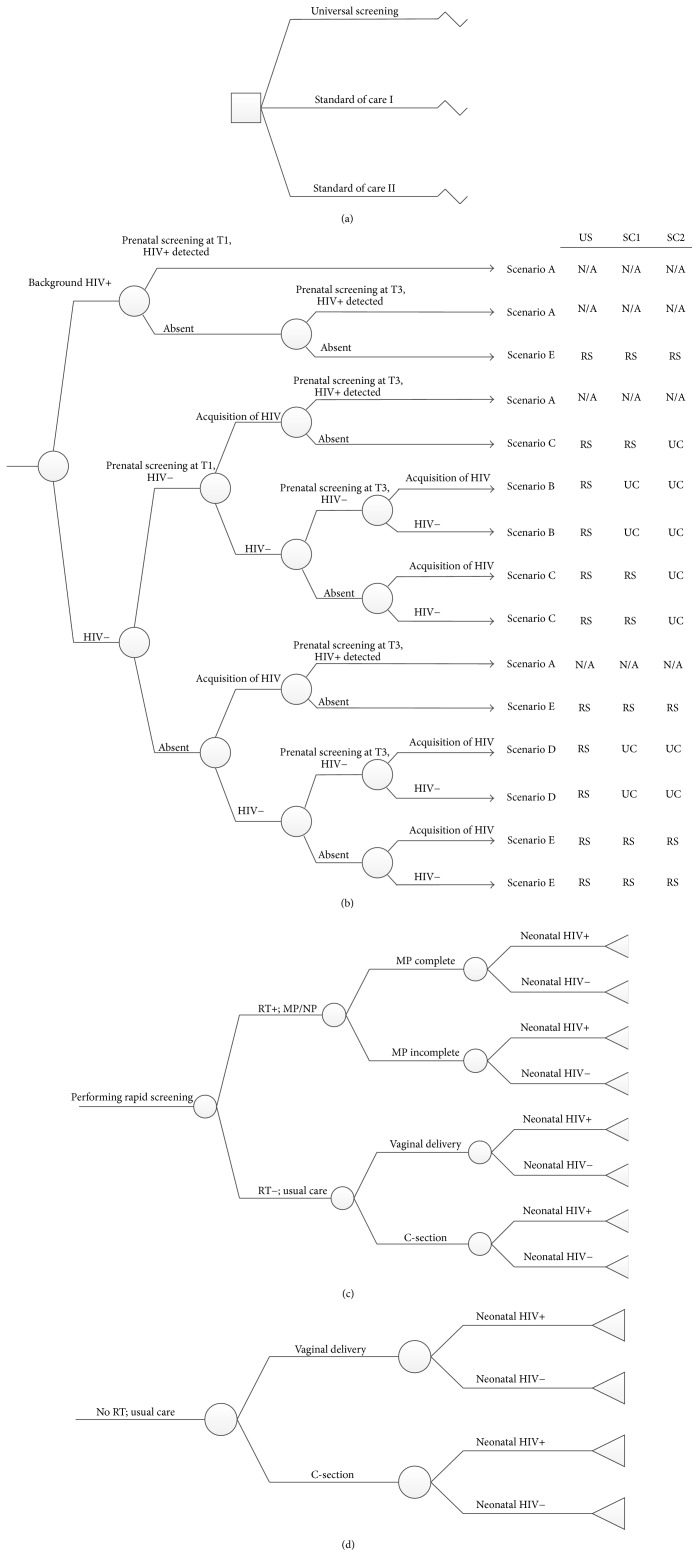
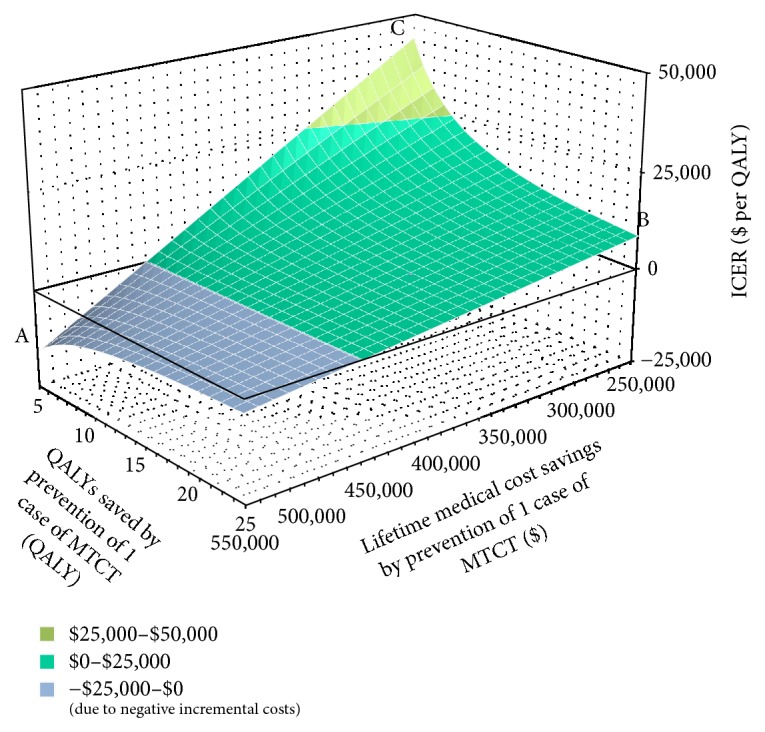
We conducted a cost-effectiveness analysis to compare the cost and QALY of universal intrapartum rapid HIV screening with two current standards of care: (I) opt-out rapid HIV testing limited to patients without previous third-trimester screening and (II) opt-out rapid HIV testing limited to patients without any prenatal screening. We developed a decision-tree model and performed sensitivity analyses to estimate the impact of variances in QALY, estimated lifetime medical costs, HIV prevalence, and cumulative incidence.
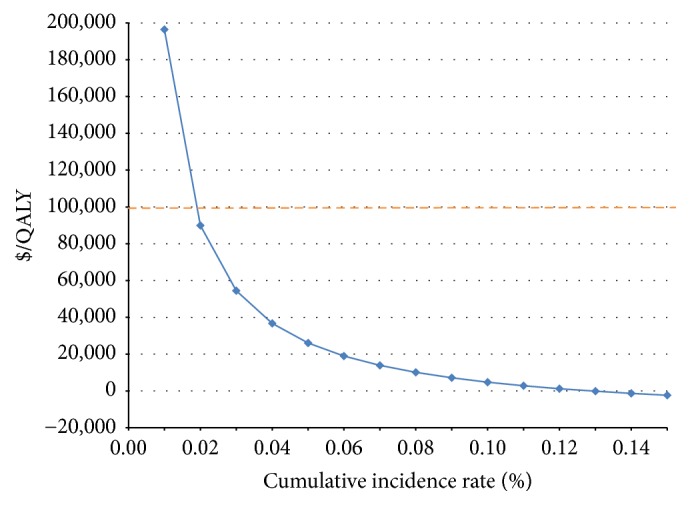
The incremental cost-effectiveness ratio for universal screening was $7,973.45/QALY. The results remained robust to sensitivity analysis, except for annual cumulative incidence. In areas with an annual cumulative incidence rate of <0.02% for reproductive-age women, the incremental cost-effectiveness ratio for the expanded program would exceed $89,926.94/QALY, approaching the commonly applied cost-effectiveness thresholds ($100,000/QALY).
Intrapartum universal rapid HIV screening to decrease MTCT appears cost-effective in populations with high HIV incidence in the United States.
通过比较分娩时普遍进行HIV快速筛查与美国目前两种产前HIV筛查护理标准的成本和质量调整生命年(QALY),确定分娩时进行普遍孕产妇HIV筛查以降低母婴传播(MTCT)的成本效益。
我们进行了一项成本效益分析,以比较分娩时普遍进行快速HIV筛查与两种当前护理标准的成本和QALY:(I)仅对未在孕晚期进行过筛查的患者进行选择退出式快速HIV检测,以及(II)仅对未进行过任何产前筛查的患者进行选择退出式快速HIV检测。我们开发了一个决策树模型,并进行了敏感性分析,以估计QALY、估计的终身医疗成本、HIV患病率和累积发病率差异的影响。
普遍筛查的增量成本效益比为7973.45美元/QALY。除年度累积发病率外,结果对敏感性分析保持稳健。在育龄妇女年度累积发病率<0.02%的地区,扩大项目的增量成本效益比将超过89926.94美元/QALY,接近常用的成本效益阈值(100000美元/QALY)。
在美国HIV发病率高的人群中,分娩时普遍进行快速HIV筛查以降低MTCT似乎具有成本效益。