Department of Global Health, University of Washington, Seattle, Washington, United States of America.
Department of Epidemiology, University of Washington, Seattle, Washington, United States of America.
PLoS Med. 2014 Feb 25;11(2):e1001608. doi: 10.1371/journal.pmed.1001608. eCollection 2014 Feb.
Women may have persistent risk of HIV acquisition during pregnancy and postpartum. Estimating risk of HIV during these periods is important to inform optimal prevention approaches. We performed a systematic review and meta-analysis to estimate maternal HIV incidence during pregnancy/postpartum and to compare mother-to-child HIV transmission (MTCT) risk among women with incident versus chronic infection.
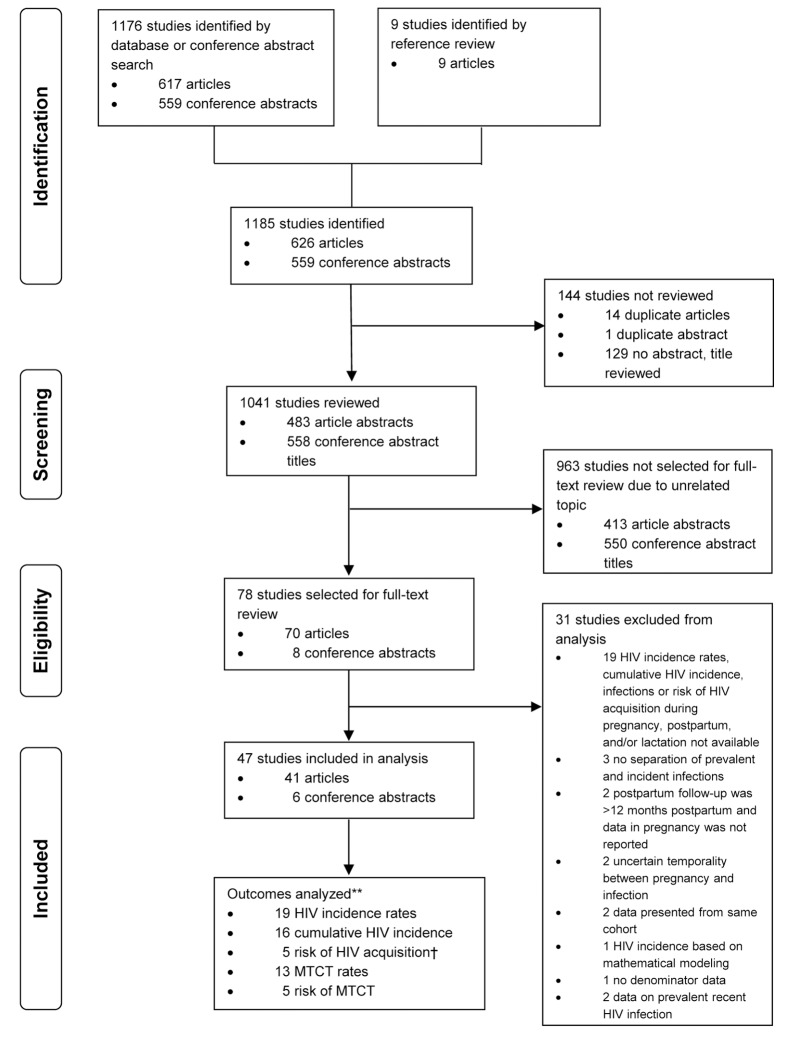
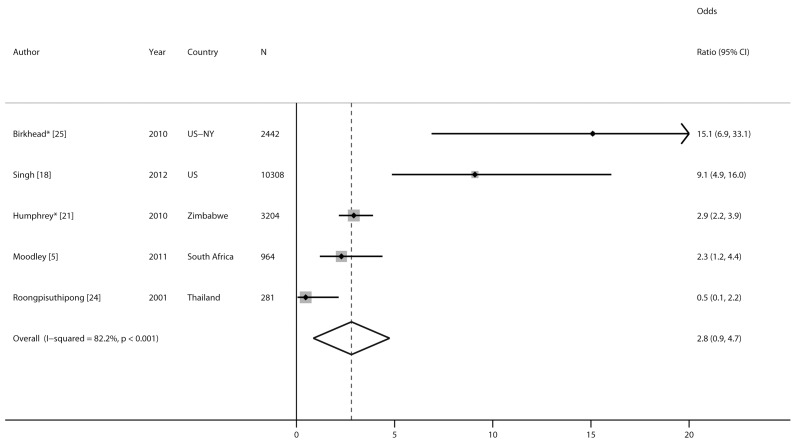
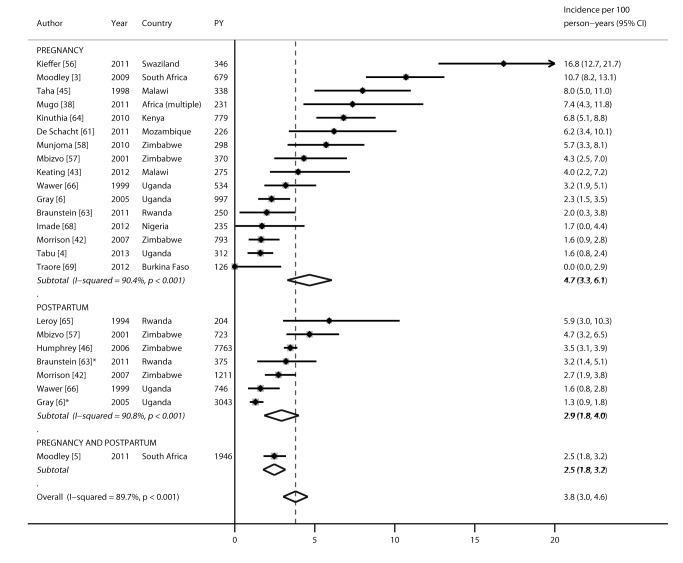
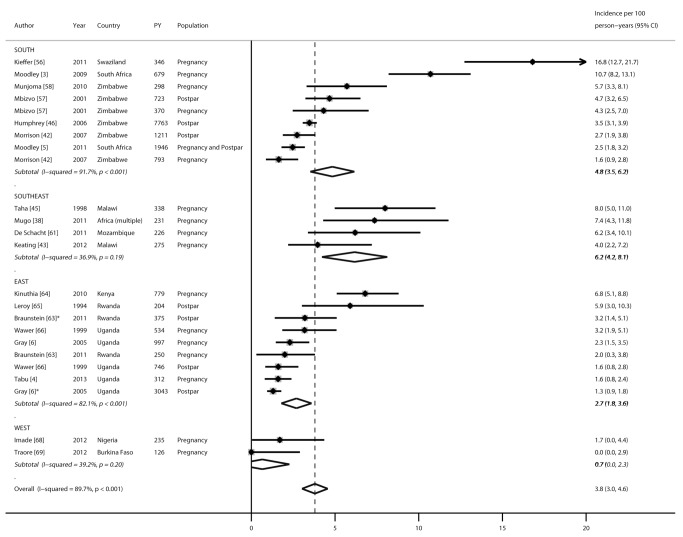
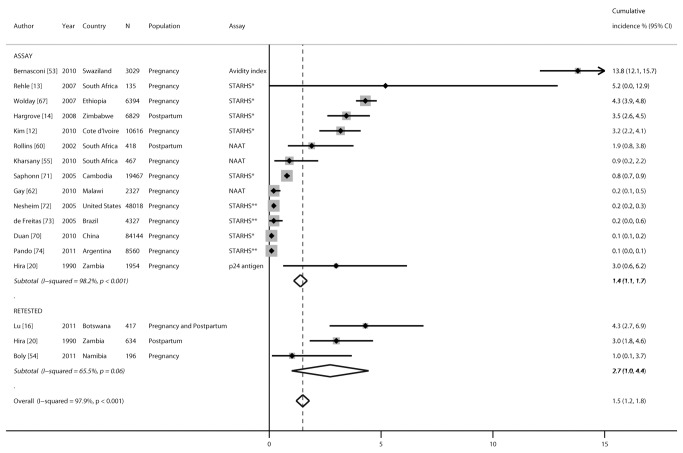
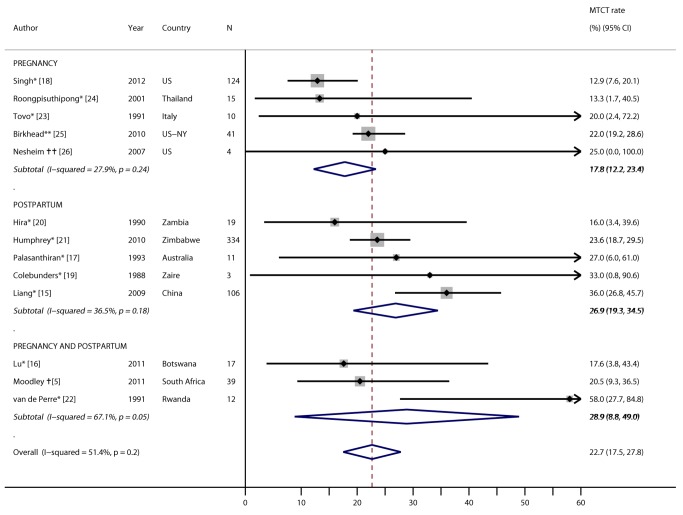
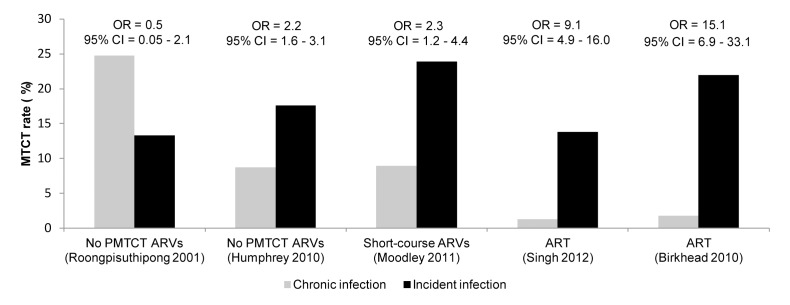
We searched PubMed, Embase, and AIDS-related conference abstracts between January 1, 1980, and October 31, 2013, for articles and abstracts describing HIV acquisition during pregnancy/postpartum. The inclusion criterion was studies with data on recent HIV during pregnancy/postpartum. Random effects models were constructed to pool HIV incidence rates, cumulative HIV incidence, hazard ratios (HRs), or odds ratios (ORs) summarizing the association between pregnancy/postpartum status and HIV incidence, and MTCT risk and rates. Overall, 1,176 studies met the search criteria, of which 78 met the inclusion criterion, and 47 contributed data. Using data from 19 cohorts representing 22,803 total person-years, the pooled HIV incidence rate during pregnancy/postpartum was 3.8/100 person-years (95% CI 3.0-4.6): 4.7/100 person-years during pregnancy and 2.9/100 person-years postpartum (p = 0.18). Pooled cumulative HIV incidence was significantly higher in African than non-African countries (3.6% versus 0.3%, respectively; p<0.001). Risk of HIV was not significantly higher among pregnant (HR 1.3, 95% CI 0.5-2.1) or postpartum women (HR 1.1, 95% CI 0.6-1.6) than among non-pregnant/non-postpartum women in five studies with available data. In African cohorts, MTCT risk was significantly higher among women with incident versus chronic HIV infection in the postpartum period (OR 2.9, 95% CI 2.2-3.9) or in pregnancy/postpartum periods combined (OR 2.3, 95% CI 1.2-4.4). However, the small number of studies limited power to detect associations and sources of heterogeneity.
Pregnancy and the postpartum period are times of persistent HIV risk, at rates similar to "high risk" cohorts. MTCT risk was elevated among women with incident infections. Detection and prevention of incident HIV in pregnancy/postpartum should be prioritized, and is critical to decrease MTCT.
女性在怀孕期间和产后可能持续面临 HIV 感染风险。评估这些时期的 HIV 感染风险对于确定最佳预防措施非常重要。我们进行了一项系统评价和荟萃分析,以评估怀孕期间和产后的孕产妇 HIV 发病率,并比较新发和慢性感染的母婴 HIV 传播 (MTCT) 风险。
我们在 1980 年 1 月 1 日至 2013 年 10 月 31 日期间,在 PubMed、Embase 和艾滋病相关会议摘要中搜索了描述怀孕期间和产后 HIV 感染的文章和摘要。纳入标准为研究最近有怀孕期间和产后 HIV 感染数据。我们构建了随机效应模型来汇总 HIV 发病率、累积 HIV 发病率、危险比 (HR) 或比值比 (OR),以总结怀孕期间和产后状态与 HIV 发病率之间的关系,以及 MTCT 风险和发生率。总的来说,有 1176 项研究符合检索标准,其中 78 项符合纳入标准,47 项提供了数据。我们使用了代表 22803 人年的 19 个队列的数据,怀孕期间和产后的 HIV 发病率分别为 3.8/100 人年(95%CI 3.0-4.6):怀孕时为 4.7/100 人年,产后为 2.9/100 人年(p=0.18)。非洲国家的累积 HIV 发病率明显高于非非洲国家(分别为 3.6%和 0.3%;p<0.001)。在有可用数据的五项研究中,孕妇(HR 1.3,95%CI 0.5-2.1)或产后妇女(HR 1.1,95%CI 0.6-1.6)的 HIV 风险并不明显高于非妊娠/非产后妇女。在非洲队列中,在产后(OR 2.9,95%CI 2.2-3.9)或怀孕期间和产后(OR 2.3,95%CI 1.2-4.4)期间,新发和慢性 HIV 感染的妇女 MTCT 风险明显更高。然而,研究数量较少限制了检测关联和异质性来源的能力。
怀孕期间和产后是 HIV 持续存在风险的时期,其风险率与“高危”队列相似。新发感染的妇女 MTCT 风险较高。在怀孕期间和产后应优先检测和预防新发 HIV,这对于降低 MTCT 至关重要。