Oxford Transplant Centre, Nuffield Department of Surgical Sciences, University of Oxford, Oxford, UK.
Institute of Biomedical Engineering, University of Oxford, Oxford, UK.
Am J Transplant. 2019 Jan;19(1):178-192. doi: 10.1111/ajt.14932. Epub 2018 Jun 20.
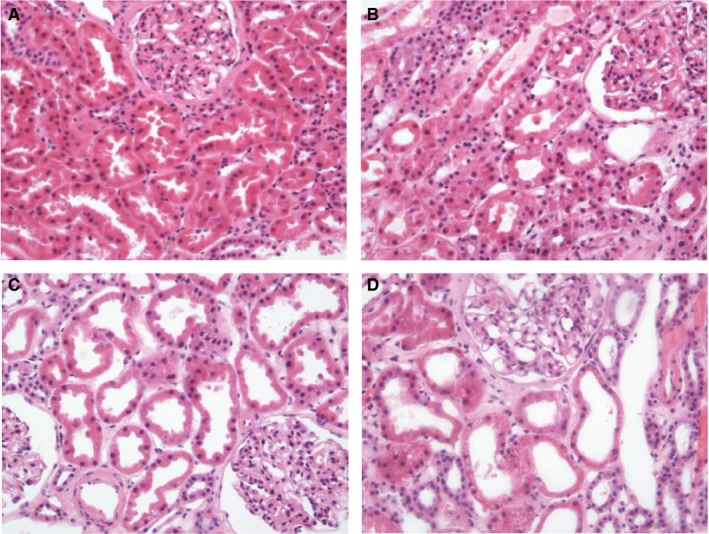
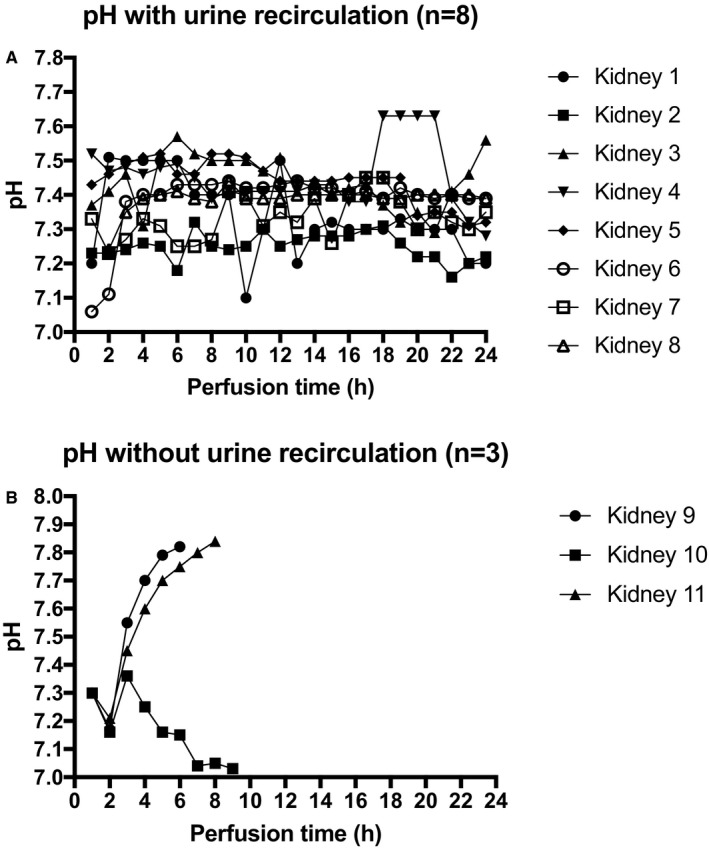
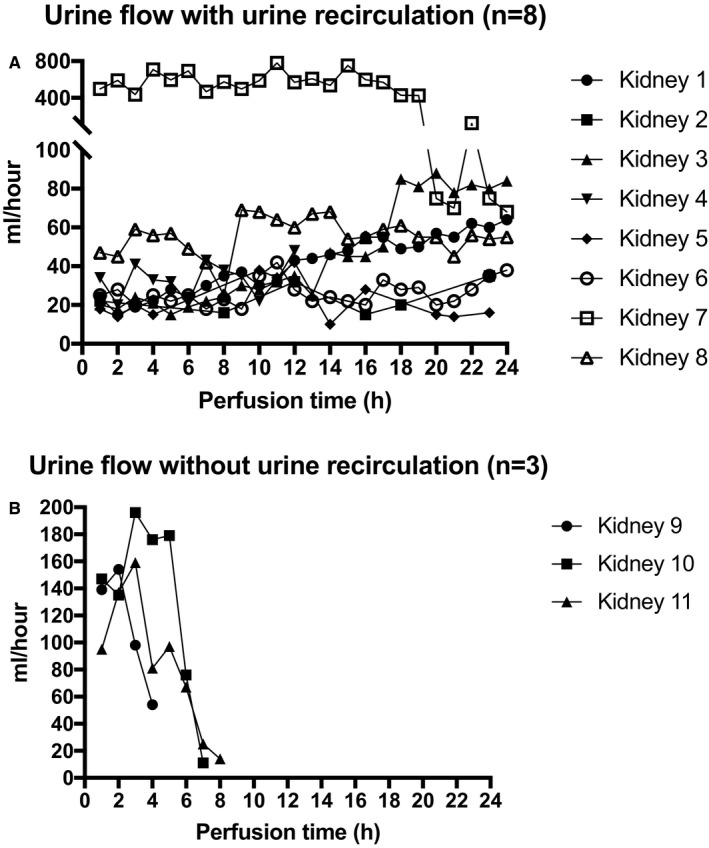
Transportable normothermic kidney perfusion for 24 hours or longer could enable viability assessment of marginal grafts, increased organ use, and improved transplant logistics. Eleven clinically declined kidneys were perfused normothermically, with 6 being from donors after brain death (median cold ischemia time 33 ± 36.9 hours) and 5 being from donors after circulatory death (36.2 ± 38.3 hours). Three kidneys were perfused using Ringer's lactate to replace excreted urine volume, and 8 kidneys were perfused using urine recirculation to maintain perfusate volume without fluid replenishment. In all cases, normothermic perfusion either maintained or slightly improved the histopathologically assessed tubular condition, and there was effective urine production in kidneys from both donors after brain death and donors after circulatory death (2367 ± 1798 mL vs 744.4 ± 198.4 mL, respectively; P = .44). Biomarkers, neutrophil gelatinase-associated lipocalin, and kidney injury molecule-1 were successfully detected and quantified in the perfusate. All kidneys with urine recirculation were readily perfused for 24 hours (n = 8) and exhibited physiological perfusate sodium levels (140.7 ± 1.2 mmol/L), while kidneys without urine recirculation (n = 3) achieved a reduced normothermic perfusion time of 7.7 ± 1.5 hours and significantly higher perfusate sodium levels (159.6 ± 4.63 mmol/:, P < .01). Normothermic machine perfusion of human kidneys for 24 hours appears to be feasible, and urine recirculation was found to facilitate the maintenance of perfusate volume and homeostasis.
可在 24 小时或更长时间内进行常温肾脏灌注,这可以实现对边缘供体的活力评估、增加器官利用率和改善移植物流。对 11 个临床宣告无法使用的肾脏进行了常温灌注,其中 6 个来自脑死亡供体(冷缺血时间中位数 33±36.9 小时),5 个来自循环死亡供体(36.2±38.3 小时)。3 个肾脏使用乳酸林格氏液替代排出的尿量进行灌注,8 个肾脏使用尿液再循环来维持灌注液量而无需补液。在所有情况下,常温灌注均维持或略微改善了组织病理学评估的肾小管状态,并且脑死亡供体和循环死亡供体的肾脏均能有效产生尿液(分别为 2367±1798ml 和 744.4±198.4ml;P=0.44)。成功地在灌注液中检测和定量了中性粒细胞明胶酶相关脂质运载蛋白和肾损伤分子-1 这两种生物标志物。所有进行尿液再循环的肾脏都可以轻松地进行 24 小时灌注(n=8),并表现出生理性的灌注液钠水平(140.7±1.2mmol/L),而没有进行尿液再循环的肾脏(n=3)仅实现了 7.7±1.5 小时的常温灌注,并且灌注液钠水平显著升高(159.6±4.63mmol/L,P<0.01)。对人类肾脏进行 24 小时常温机器灌注似乎是可行的,并且发现尿液再循环有助于维持灌注液量和内环境稳定。