Bousema Jelle E, Dijkgraaf Marcel G W, Papen-Botterhuis Nicole E, Schreurs Hermien W, Maessen Jos G, van der Heijden Erik H, Steup Willem H, Braun Jerry, Noyez Valentin J J M, Hoeijmakers Fieke, Beck Naomi, van Dorp Martijn, Claessens Niels J M, Hiddinga Birgitta I, Daniels Johannes M A, Heineman David J, Zandbergen Harmen R, Verhagen Ad F T M, van Schil Paul E, Annema Jouke T, van den Broek Frank J C
Department of Surgery, Máxima Medical Center, PO BOX 7777, 5500 MB, Veldhoven, the Netherlands.
University of Amsterdam, Amsterdam, the Netherlands.
BMC Surg. 2018 May 18;18(1):27. doi: 10.1186/s12893-018-0359-6.
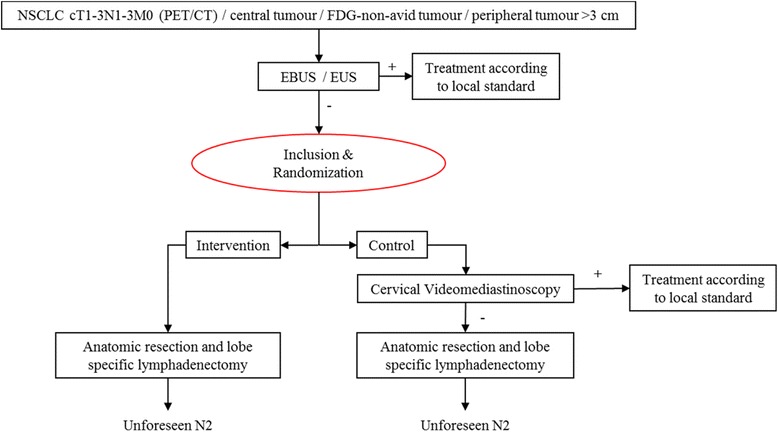
In case of suspicious lymph nodes on computed tomography (CT) or fluorodeoxyglucose positron emission tomography (FDG-PET), advanced tumour size or central tumour location in patients with suspected non-small cell lung cancer (NSCLC), Dutch and European guidelines recommend mediastinal staging by endosonography (endobronchial ultrasound (EBUS) and endoscopic ultrasound (EUS)) with sampling of mediastinal lymph nodes. If biopsy results from endosonography turn out negative, additional surgical staging of the mediastinum by mediastinoscopy is advised to prevent unnecessary lung resection due to false negative endosonography findings. We hypothesize that omitting mediastinoscopy after negative endosonography in mediastinal staging of NSCLC does not result in an unacceptable percentage of unforeseen N2 disease at surgical resection. In addition, omitting mediastinoscopy comprises no extra waiting time until definite surgery, omits one extra general anaesthesia and hospital admission, and may be associated with lower morbidity and comparable survival. Therefore, this strategy may reduce health care costs and increase quality of life. The aim of this study is to compare the cost-effectiveness and cost-utility of mediastinal staging strategies including and excluding mediastinoscopy.
METHODS/DESIGN: This study is a multicenter parallel randomized non-inferiority trial comparing two diagnostic strategies (with or without mediastinoscopy) for mediastinal staging in 360 patients with suspected resectable NSCLC. Patients are eligible for inclusion when they underwent systematic endosonography to evaluate mediastinal lymph nodes including tissue sampling with negative endosonography results. Patients will not be eligible for inclusion when PET/CT demonstrates 'bulky N2-N3' disease or the combination of a highly suspicious as well as irresectable mediastinal lymph node. Primary outcome measure for non-inferiority is the proportion of patients with unforeseen N2 disease at surgery. Secondary outcome measures are hospitalization, morbidity, overall 2-year survival, quality of life, cost-effectiveness and cost-utility. Patients will be followed up 2 years after start of treatment.
Results of the MEDIASTrial will have immediate impact on national and international guidelines, which are accessible to public, possibly reducing mediastinoscopy as a commonly performed invasive procedure for NSCLC staging and diminishing variation in clinical practice.
The trial is registered at the Netherlands Trial Register on July 6th, 2017 ( NTR 6528 ).
对于计算机断层扫描(CT)或氟脱氧葡萄糖正电子发射断层扫描(FDG-PET)显示可疑淋巴结、肿瘤大小较大或肿瘤位于中央的疑似非小细胞肺癌(NSCLC)患者,荷兰和欧洲指南建议通过内镜超声检查(支气管内超声(EBUS)和内镜超声(EUS))进行纵隔分期,并对纵隔淋巴结进行采样。如果内镜超声检查的活检结果为阴性,建议通过纵隔镜检查对纵隔进行额外的手术分期,以防止因内镜超声检查结果假阴性而进行不必要的肺切除术。我们假设,在NSCLC纵隔分期中,内镜超声检查结果为阴性后省略纵隔镜检查不会导致手术切除时意外N2期疾病的比例不可接受。此外,省略纵隔镜检查不会增加直至明确手术的额外等待时间,省略一次额外的全身麻醉和住院,并且可能与较低的发病率和相当的生存率相关。因此,这种策略可能会降低医疗成本并提高生活质量。本研究的目的是比较包括和不包括纵隔镜检查的纵隔分期策略的成本效益和成本效用。
方法/设计:本研究是一项多中心平行随机非劣效性试验,比较360例疑似可切除NSCLC患者纵隔分期的两种诊断策略(有无纵隔镜检查)。当患者接受系统的内镜超声检查以评估纵隔淋巴结,包括组织采样且内镜超声检查结果为阴性时,符合纳入条件。当PET/CT显示“巨大N2-N3”疾病或高度可疑且不可切除的纵隔淋巴结合并存在时,患者不符合纳入条件。非劣效性的主要结局指标是手术时意外N2期疾病患者的比例。次要结局指标包括住院、发病率、总体2年生存率、生活质量、成本效益和成本效用。患者将在治疗开始后随访2年。
MEDIASTrial的结果将对国家和国际指南产生直接影响,这些指南可供公众获取,可能会减少纵隔镜检查作为NSCLC分期常用的侵入性程序,并减少临床实践中的差异。
该试验于2017年7月6日在荷兰试验注册中心注册(NTR 6528)。