Stroke Trials Unit, Division of Clinical Neuroscience, University of Nottingham, City Hospital Campus, Nottingham, UK; Stroke, Nottingham University Hospitals NHS Trust, City Hospital Campus, Nottingham, UK.
Stroke Trials Unit, Division of Clinical Neuroscience, University of Nottingham, City Hospital Campus, Nottingham, UK.
Lancet. 2018 May 26;391(10135):2107-2115. doi: 10.1016/S0140-6736(18)31033-X. Epub 2018 May 16.
Tranexamic acid can prevent death due to bleeding after trauma and post-partum haemorrhage. We aimed to assess whether tranexamic acid reduces haematoma expansion and improves outcome in adults with stroke due to intracerebral haemorrhage.
We did an international, randomised placebo-controlled trial in adults with intracerebral haemorrhage from acute stroke units at 124 hospital sites in 12 countries. Participants were randomly assigned (1:1) to receive 1 g intravenous tranexamic acid bolus followed by an 8 h infusion of 1 g tranexamic acid or a matching placebo, within 8 h of symptom onset. Randomisation was done centrally in real time via a secure website, with stratification by country and minimisation on key prognostic factors. Treatment allocation was concealed from patients, outcome assessors, and all other health-care workers involved in the trial. The primary outcome was functional status at day 90, measured by shift in the modified Rankin Scale, using ordinal logistic regression with adjustment for stratification and minimisation criteria. All analyses were done on an intention-to-treat basis. This trial is registered with the ISRCTN registry, number ISRCTN93732214.
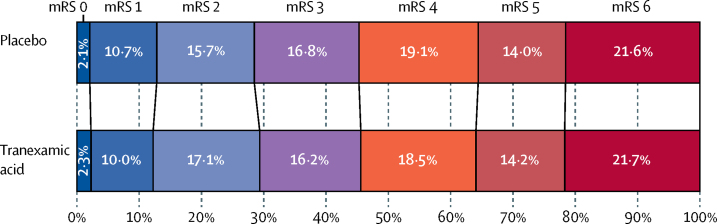
We recruited 2325 participants between March 1, 2013, and Sept 30, 2017. 1161 patients received tranexamic acid and 1164 received placebo; the treatment groups were well balanced at baseline. The primary outcome was assessed for 2307 (99%) participants. The primary outcome, functional status at day 90, did not differ significantly between the groups (adjusted odds ratio [aOR] 0·88, 95% CI 0·76-1·03, p=0·11). Although there were fewer deaths by day 7 in the tranexamic acid group (101 [9%] deaths in the tranexamic acid group vs 123 [11%] deaths in the placebo group; aOR 0·73, 0·53-0·99, p=0·0406), there was no difference in case fatality at 90 days (250 [22%] vs 249 [21%]; adjusted hazard ratio 0·92, 95% CI 0·77-1·10, p=0·37). Fewer patients had serious adverse events after tranexamic acid than after placebo by days 2 (379 [33%] patients vs 417 [36%] patients), 7 (456 [39%] vs 497 [43%]), and 90 (521 [45%] vs 556 [48%]).
Functional status 90 days after intracerebral haemorrhage did not differ significantly between patients who received tranexamic acid and those who received placebo, despite a reduction in early deaths and serious adverse events. Larger randomised trials are needed to confirm or refute a clinically significant treatment effect.
National Institute of Health Research Health Technology Assessment Programme and Swiss Heart Foundation.
氨甲环酸可预防创伤后和产后出血导致的死亡。我们旨在评估氨甲环酸是否可减少因脑出血导致的中风患者的血肿扩大并改善其结局。
我们在 12 个国家的 124 家医院的急性中风病房进行了一项国际性、随机、安慰剂对照试验。参与者在症状发作后 8 小时内被随机(1:1)分配接受 1g 静脉氨甲环酸推注,然后输注 8 小时 1g 氨甲环酸或匹配的安慰剂。通过一个安全的网站实时进行中心随机化,按国家和最小化关键预后因素分层。治疗分配对患者、结局评估者和参与试验的所有其他医护人员均保密。主要结局是第 90 天时的功能状态,使用改良 Rankin 量表的变化进行评估,采用有序逻辑回归进行分析,并调整了分层和最小化标准。所有分析均基于意向治疗原则进行。该试验在 ISRCTN 注册中心注册,编号为 ISRCTN93732214。
我们于 2013 年 3 月 1 日至 2017 年 9 月 30 日期间招募了 2325 名参与者。1161 名患者接受了氨甲环酸治疗,1164 名患者接受了安慰剂治疗;两组在基线时具有良好的均衡性。2307 名(99%)参与者评估了主要结局。主要结局,即第 90 天时的功能状态,两组之间无显著差异(校正比值比 [aOR] 0·88,95%CI 0·76-1·03,p=0·11)。虽然氨甲环酸组在第 7 天的死亡率较低(氨甲环酸组 101 例[9%]死亡,安慰剂组 123 例[11%]死亡;aOR 0·73,0·53-0·99,p=0·0406),但 90 天时的病死率无差异(氨甲环酸组 250 例[22%]死亡,安慰剂组 249 例[21%]死亡;调整后的危险比 0·92,95%CI 0·77-1·10,p=0·37)。与安慰剂相比,氨甲环酸组在第 2 天(379 例[33%]患者比 417 例[36%]患者)、第 7 天(456 例[39%]患者比 497 例[43%]患者)和第 90 天(521 例[45%]患者比 556 例[48%]患者)的严重不良事件更少。
尽管氨甲环酸可降低早期死亡和严重不良事件的发生率,但脑出血后 90 天时接受氨甲环酸治疗和安慰剂治疗的患者的功能状态无显著差异。需要更大规模的随机试验来证实或反驳氨甲环酸治疗的临床显著效果。
英国国家卫生与保健优化研究所卫生技术评估计划和瑞士心脏基金会。