Gayet-Ageron Angèle, Prieto-Merino David, Ker Katharine, Shakur Haleema, Ageron François-Xavier, Roberts Ian
Clinical Trials Unit, London School of Hygiene & Tropical Medicine, London, UK; Division of Clinical Epidemiology, University Hospitals of Geneva, Geneva, Switzerland.
Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK.
Lancet. 2018 Jan 13;391(10116):125-132. doi: 10.1016/S0140-6736(17)32455-8. Epub 2017 Nov 7.
Antifibrinolytics reduce death from bleeding in trauma and post-partum haemorrhage. We examined the effect of treatment delay on the effectiveness of antifibrinolytics.
We did an individual patient-level data meta-analysis of randomised trials done with more than 1000 patients that assessed antifibrinolytics in acute severe bleeding. We identified trials done between Jan 1, 1946, and April 7, 2017, from MEDLINE, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, PubMed, Popline, and the WHO International Clinical Trials Registry Platform. The primary measure of treatment benefit was absence of death from bleeding. We examined the effect of treatment delay on treatment effectiveness using logistic regression models. We investigated the effect of measurement error (misclassification) in sensitivity analyses. This study is registered with PROSPERO, number 42016052155.
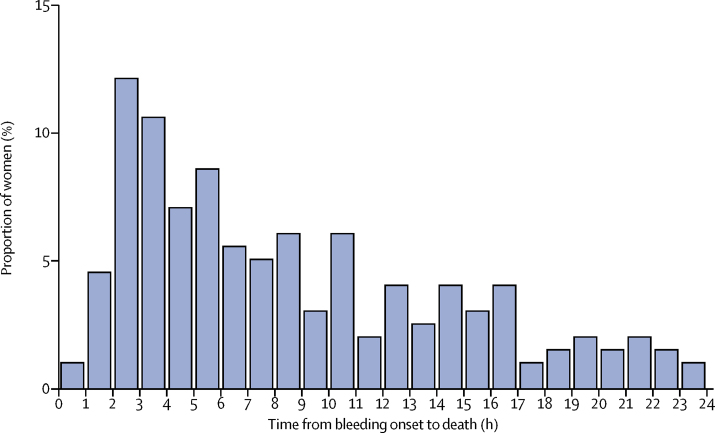
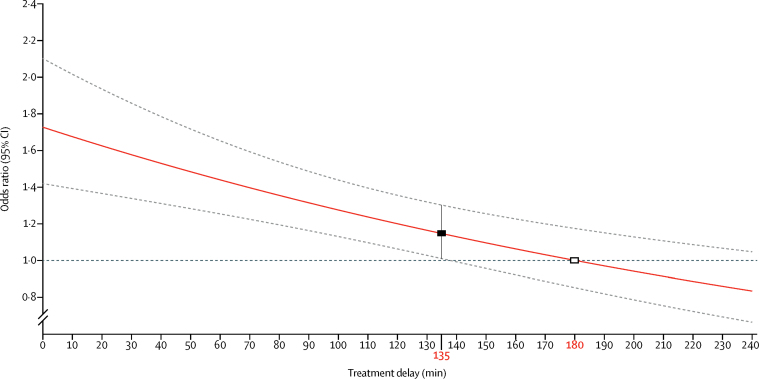
We obtained data for 40 138 patients from two randomised trials of tranexamic acid in acute severe bleeding (traumatic and post-partum haemorrhage). Overall, there were 3558 deaths, of which 1408 (40%) were from bleeding. Most (884 [63%] of 1408) bleeding deaths occurred within 12 h of onset. Deaths from post-partum haemorrhage peaked 2-3 h after childbirth. Tranexamic acid significantly increased overall survival from bleeding (odds ratio [OR] 1·20, 95% CI 1·08-1·33; p=0·001), with no heterogeneity by site of bleeding (interaction p=0·7243). Treatment delay reduced the treatment benefit (p<0·0001). Immediate treatment improved survival by more than 70% (OR 1·72, 95% CI 1·42-2·10; p<0·0001). Thereafter, the survival benefit decreased by 10% for every 15 min of treatment delay until 3 h, after which there was no benefit. There was no increase in vascular occlusive events with tranexamic acid, with no heterogeneity by site of bleeding (p=0·5956). Treatment delay did not modify the effect of tranexamic acid on vascular occlusive events.
Death from bleeding occurs soon after onset and even a short delay in treatment reduces the benefit of tranexamic acid administration. Patients must be treated immediately. Further research is needed to deepen our understanding of the mechanism of action of tranexamic acid.
UK NIHR Health Technology Assessment programme, Pfizer, BUPA Foundation, and J P Moulton Charitable Foundation (CRASH-2 trial). London School of Hygiene & Tropical Medicine, Pfizer, UK Department of Health, Wellcome Trust, and Bill & Melinda Gates Foundation (WOMAN trial).
抗纤溶药物可降低创伤和产后出血导致的死亡风险。我们研究了治疗延迟对抗纤溶药物疗效的影响。
我们对超过1000例患者的随机试验进行了个体患者水平的数据荟萃分析,这些试验评估了抗纤溶药物在急性严重出血中的应用。我们从MEDLINE、Embase、Cochrane对照试验中央注册库(CENTRAL)、科学网、PubMed、Popline和世界卫生组织国际临床试验注册平台中检索了1946年1月1日至2017年4月7日期间开展的试验。治疗获益的主要衡量指标是无出血死亡。我们使用逻辑回归模型研究治疗延迟对治疗效果的影响。我们在敏感性分析中调查了测量误差(错误分类)的影响。本研究已在国际前瞻性系统评价注册库(PROSPERO)注册,注册号为42016052155。
我们从两项关于氨甲环酸治疗急性严重出血(创伤性和产后出血)的随机试验中获得了40138例患者的数据。总体而言,共有3558例死亡,其中1408例(40%)死于出血。大多数(1408例中的884例[63%])出血死亡发生在发病后12小时内。产后出血导致的死亡在分娩后2 - 3小时达到峰值。氨甲环酸显著提高了出血导致的总体生存率(比值比[OR]为1.20,95%置信区间为1.08 - 1.33;p = 0.001),不同出血部位之间无异质性(交互作用p = 0.7243)。治疗延迟降低了治疗获益(p < 0.0001)。立即治疗使生存率提高了70%以上(OR为1.72,95%置信区间为1.42 - 2.10;p < 0.0001)。此后,每延迟治疗15分钟,生存获益就降低10%,直至3小时,此后则无获益。氨甲环酸并未增加血管闭塞事件的发生,不同出血部位之间无异质性(p = 0.5956)。治疗延迟并未改变氨甲环酸对血管闭塞事件的影响。
出血导致的死亡在发病后很快发生,即使治疗稍有延迟也会降低氨甲环酸给药的获益。必须立即对患者进行治疗。需要进一步研究以加深我们对氨甲环酸作用机制的理解。
英国国家卫生研究院卫生技术评估项目、辉瑞公司、保柏基金会和J·P·莫尔顿慈善基金会(CRASH - 2试验)。伦敦卫生与热带医学学院、辉瑞公司、英国卫生部、惠康信托基金会和比尔及梅琳达·盖茨基金会(WOMAN试验)。