Department of Medicine, Stanford University School of Medicine, Stanford, CA.
New York University School of Medicine, New York, New York.
Am Heart J. 2018 Jul;201:124-135. doi: 10.1016/j.ahj.2018.04.011. Epub 2018 Apr 21.
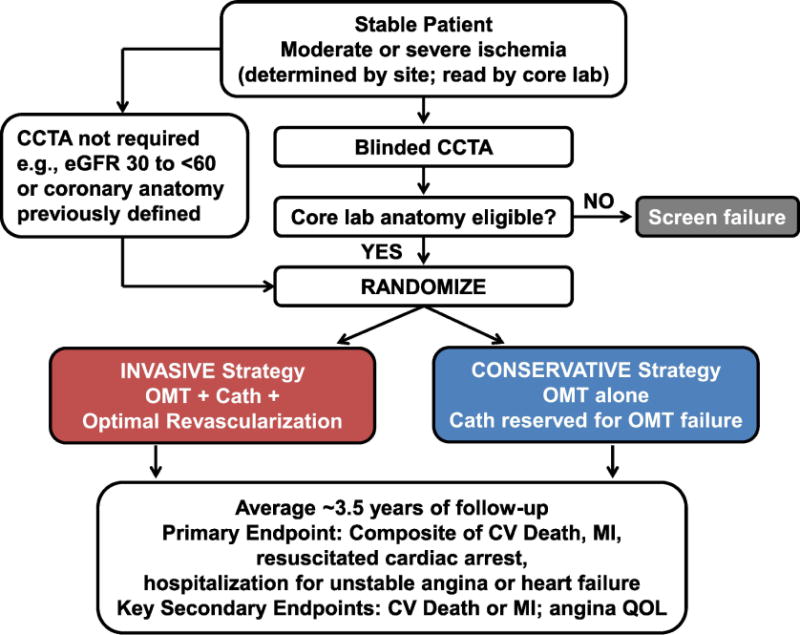
Prior trials comparing a strategy of optimal medical therapy with or without revascularization have not shown that revascularization reduces cardiovascular events in patients with stable ischemic heart disease (SIHD). However, those trials only included participants in whom coronary anatomy was known prior to randomization and did not include sufficient numbers of participants with significant ischemia. It remains unknown whether a routine invasive approach offers incremental value over a conservative approach with catheterization reserved for failure of medical therapy in patients with moderate or severe ischemia.
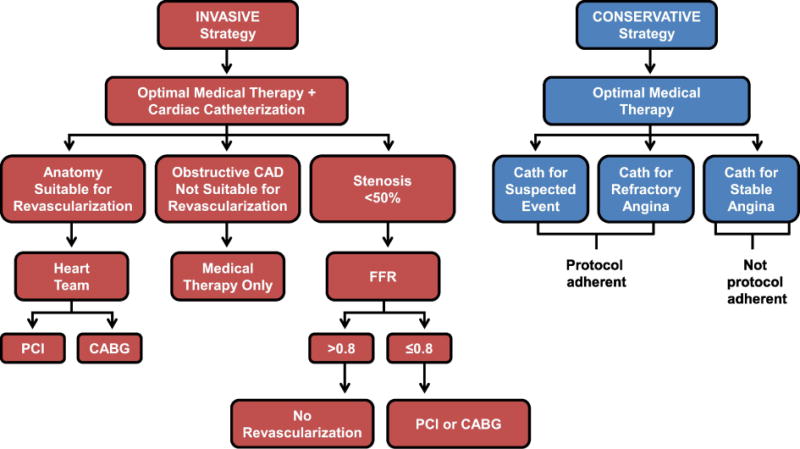
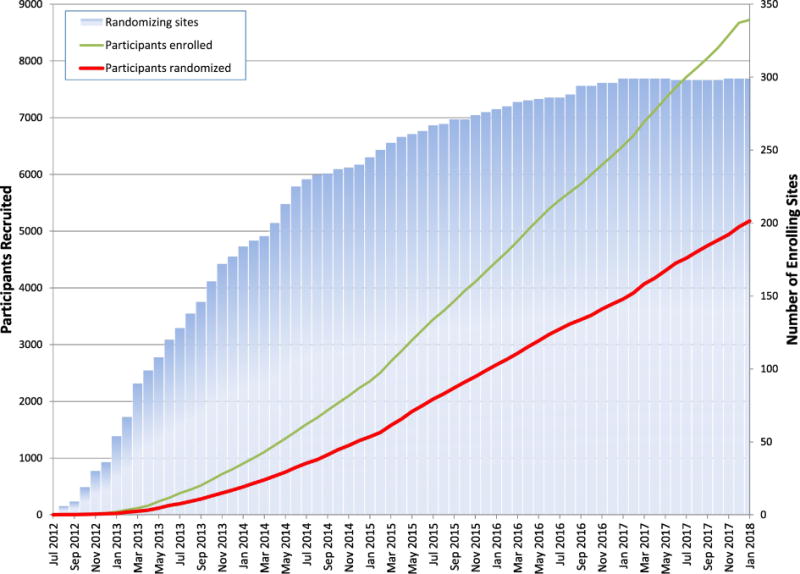
The ISCHEMIA trial is a National Heart, Lung, and Blood Institute supported trial, designed to compare an initial invasive or conservative treatment strategy for managing SIHD patients with moderate or severe ischemia on stress testing. Five thousand one-hundred seventy-nine participants have been randomized. Key exclusion criteria included estimated glomerular filtration rate (eGFR) <30 mL/min, recent myocardial infarction (MI), left ventricular ejection fraction <35%, left main stenosis >50%, or unacceptable angina at baseline. Most enrolled participants with normal renal function first underwent blinded coronary computed tomography angiography (CCTA) to exclude those with left main coronary artery disease (CAD) and without obstructive CAD. All randomized participants receive secondary prevention that includes lifestyle advice and pharmacologic interventions referred to as optimal medical therapy (OMT). Participants randomized to the invasive strategy underwent routine cardiac catheterization followed by revascularization with percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) surgery, when feasible, as selected by the local Heart Team to achieve optimal revascularization. Participants randomized to the conservative strategy undergo cardiac catheterization only for failure of OMT. The primary endpoint is a composite of cardiovascular (CV) death, nonfatal myocardial infarction (MI), hospitalization for unstable angina, hospitalization for heart failure, or resuscitated cardiac arrest. Assuming the primary endpoint will occur in 16% of the conservative group within 4 years, estimated power exceeds 80% to detect an 18.5% reduction in the primary endpoint. Major secondary endpoints include the composite of CV death and nonfatal MI, net clinical benefit (primary and secondary endpoints combined with stroke), angina-related symptoms and disease-specific quality of life, as well as a cost-effectiveness assessment in North American participants. Ancillary studies of patients with advanced chronic kidney disease and those with documented ischemia and non-obstructive coronary artery disease are being conducted concurrently.
ISCHEMIA will provide new scientific evidence regarding whether an invasive management strategy improves clinical outcomes when added to optimal medical therapy in patients with SIHD and moderate or severe ischemia.
先前比较最佳药物治疗策略加或不加血运重建的临床试验并未显示血运重建可降低稳定性缺血性心脏病(SIHD)患者的心血管事件。然而,这些试验仅纳入了随机分组前已知冠状动脉解剖结构的参与者,且未纳入足够数量的有明显缺血的患者。在中等或重度缺血患者中,与保留用于药物治疗失败的有创性方法相比,常规有创性方法是否优于保留性方法,导管术是否具有附加价值仍不清楚。
ISCHEMIA 试验是美国国立心肺血液研究所(National Heart,Lung,and Blood Institute)支持的一项试验,旨在比较初始有创或保守治疗策略,用于管理中等或重度应激试验缺血的 SIHD 患者。5179 名参与者被随机分组。主要排除标准包括估计肾小球滤过率(eGFR)<30ml/min、近期心肌梗死(MI)、左心室射血分数(LVEF)<35%、左主干狭窄>50%或基线时不能耐受心绞痛。大多数肾功能正常的入组患者首先接受盲法冠状动脉计算机断层血管造影术(CCTA),以排除左主干冠状动脉疾病(CAD)和无阻塞性 CAD 的患者。所有随机分组的参与者均接受二级预防,包括生活方式建议和药物干预,称为最佳药物治疗(OMT)。随机分组至有创策略的参与者接受常规心脏导管术,然后根据当地心脏团队的选择进行经皮冠状动脉介入治疗(PCI)或冠状动脉旁路移植术(CABG),以实现最佳血运重建。随机分组至保守策略的参与者仅在 OMT 失败时进行心脏导管术。主要终点是心血管(CV)死亡、非致死性心肌梗死(MI)、不稳定型心绞痛住院、心力衰竭住院或复苏性心脏骤停的复合终点。假设保守组的主要终点在 4 年内将以 16%的概率发生,估计效力超过 80%,可检测到主要终点降低 18.5%。主要次要终点包括 CV 死亡和非致死性 MI 的复合终点、净临床获益(主要和次要终点与中风相结合)、与心绞痛相关的症状和疾病特异性生活质量,以及北美参与者的成本效益评估。同时进行了伴有晚期慢性肾脏病的患者以及有记录的缺血和非阻塞性 CAD 的患者的辅助研究。
ISCHEMIA 将提供新的科学证据,表明在 SIHD 和中等或重度缺血患者中,在最佳药物治疗基础上加用有创性管理策略是否可改善临床结局。