New York University School of Medicine, New York, NY.
Stanford University School of Medicine, Stanford, CA.
Am Heart J. 2018 Nov;205:42-52. doi: 10.1016/j.ahj.2018.07.023. Epub 2018 Aug 1.
Patients with chronic kidney disease (CKD) and stable ischemic heart disease are at markedly increased risk of cardiovascular events. Prior trials comparing a strategy of optimal medical therapy (OMT) with or without revascularization have largely excluded patients with advanced CKD. Whether a routine invasive approach when compared with a conservative strategy is beneficial in such patients is unknown.
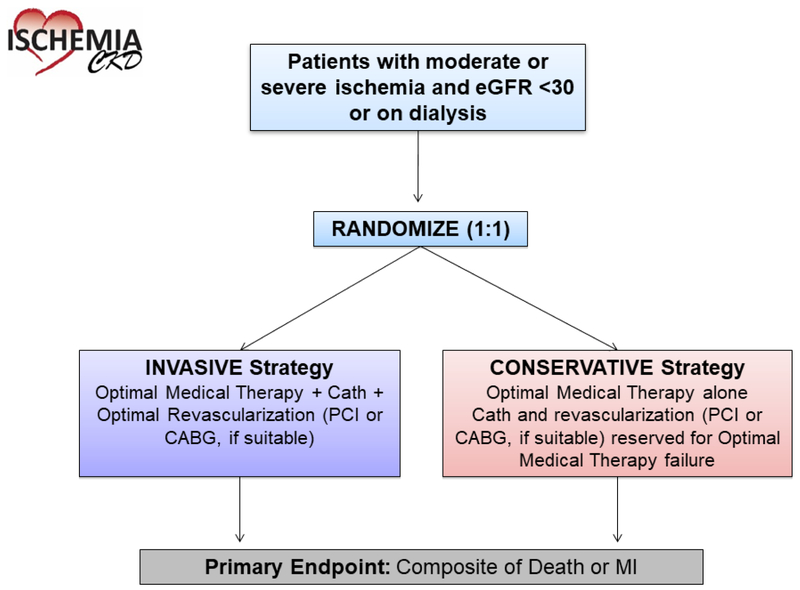
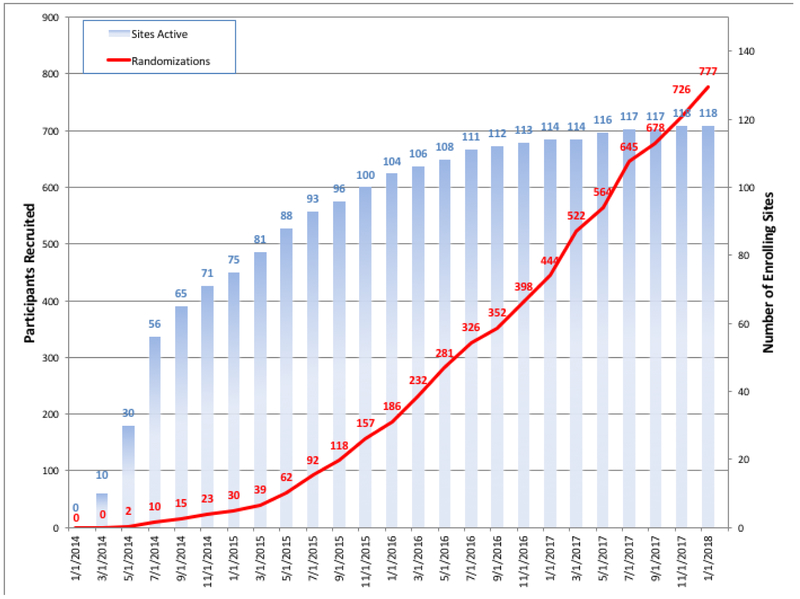
ISCHEMIA-CKD is a National Heart, Lung, and Blood Institute-funded randomized trial designed to determine the comparative effectiveness of an initial invasive strategy (cardiac catheterization and optimal revascularization [percutaneous coronary intervention or coronary artery bypass graft surgery, if suitable] plus OMT) versus a conservative strategy (OMT alone, with cardiac catheterization and revascularization [percutaneous coronary intervention or coronary artery bypass graft surgery, if suitable] reserved for failure of OMT) on long-term clinical outcomes in 777 patients with advanced CKD (defined as those with estimated glomerular filtration rate <30 mL/min/1.73m or on dialysis) and moderate or severe ischemia on stress testing. Participants were randomized in a 1:1 fashion to the invasive or a conservative strategy. The primary end point is a composite of death or nonfatal myocardial infarction. Major secondary endpoints are a composite of death, nonfatal myocardial infarction, hospitalization for unstable angina, hospitalization for heart failure, or resuscitated cardiac arrest; angina control; and disease-specific quality of life. Safety outcomes such as initiation of maintenance dialysis and a composite of initiation of maintenance dialysis or death will be reported. The trial is projected to have 80% power to detect a 22% to 24% reduction in the primary composite end point with the invasive strategy when compared with the conservative strategy.
ISCHEMIA-CKD will determine whether an initial invasive management strategy improves clinical outcomes when added to OMT in patients with advanced CKD and stable ischemic heart disease.
患有慢性肾脏病(CKD)和稳定型缺血性心脏病的患者发生心血管事件的风险明显增加。先前比较最佳药物治疗(OMT)加或不加血运重建策略的试验大多排除了晚期 CKD 患者。在这些患者中,常规侵入性方法与保守策略相比是否有益尚不清楚。
ISCHEMIA-CKD 是一项由美国国立心肺血液研究所资助的随机试验,旨在确定初始侵入性策略(心脏导管检查和最佳血运重建[经皮冠状动脉介入治疗或冠状动脉旁路移植术,如果合适]加 OMT)与保守策略(单独 OMT,心脏导管检查和血运重建[经皮冠状动脉介入治疗或冠状动脉旁路移植术,如果合适]保留用于 OMT 失败)在 777 例晚期 CKD(定义为肾小球滤过率估计值 <30 mL/min/1.73m 或透析患者)和应激试验中存在中度或重度缺血的患者中的长期临床结局比较。参与者以 1:1 的比例随机分配到侵入性或保守策略组。主要终点是死亡或非致死性心肌梗死的复合终点。主要次要终点是死亡、非致死性心肌梗死、不稳定型心绞痛住院、心力衰竭住院或复苏性心脏骤停的复合终点;心绞痛控制;和特定疾病的生活质量。将报告安全性结局,如开始维持性透析和开始维持性透析或死亡的复合终点。该试验预计有 80%的效能检测到与保守策略相比,侵入性策略可使主要复合终点降低 22%至 24%。
ISCHEMIA-CKD 将确定在晚期 CKD 和稳定型缺血性心脏病患者中,在 OMT 基础上添加初始侵入性管理策略是否改善临床结局。