Instituto de Saúde Coletiva, Universidade Federal da Bahia, Salvador, Bahia, Brazil.
Public Health Policy Evaluation Unit, Department of Primary Care and Public Health, School of Public Health, Imperial College London, London, United Kingdom.
PLoS Med. 2018 May 22;15(5):e1002570. doi: 10.1371/journal.pmed.1002570. eCollection 2018 May.
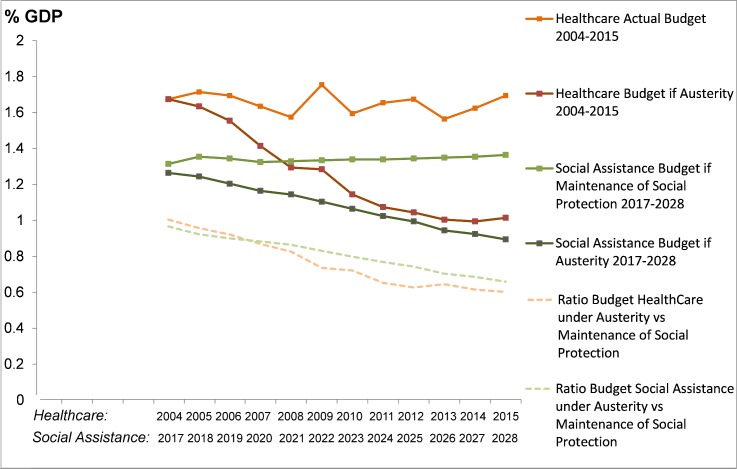
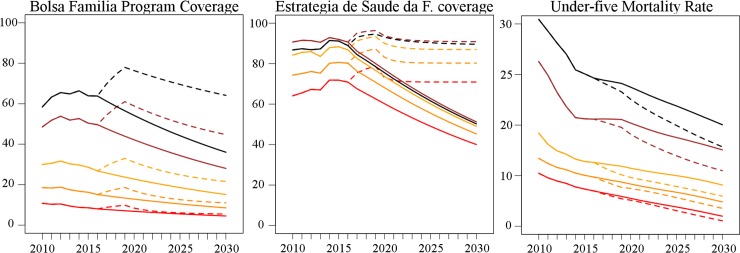
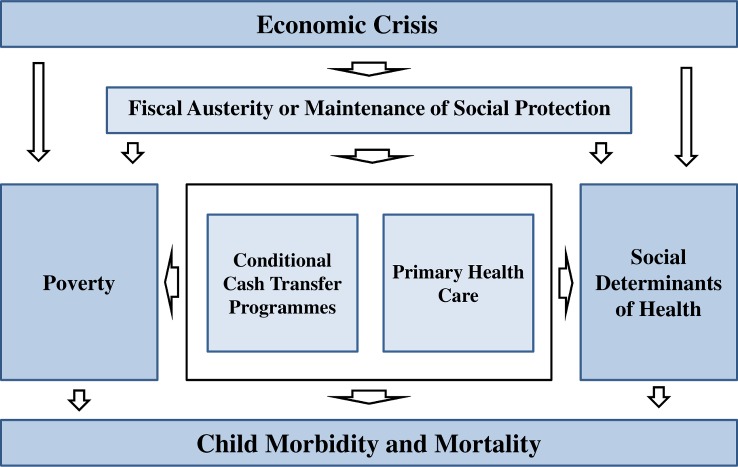
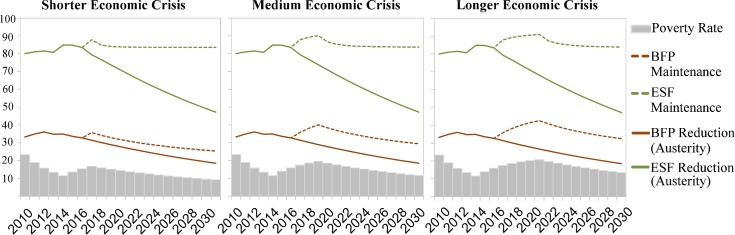
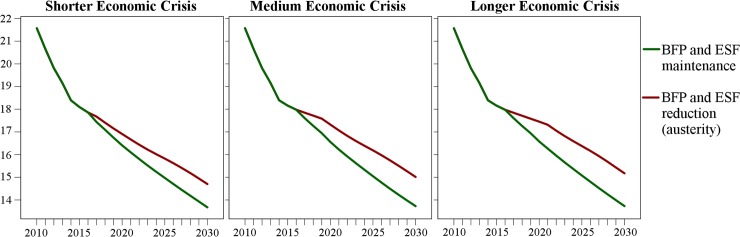
Since 2015, a major economic crisis in Brazil has led to increasing poverty and the implementation of long-term fiscal austerity measures that will substantially reduce expenditure on social welfare programmes as a percentage of the country's GDP over the next 20 years. The Bolsa Família Programme (BFP)-one of the largest conditional cash transfer programmes in the world-and the nationwide primary healthcare strategy (Estratégia Saúde da Família [ESF]) are affected by fiscal austerity, despite being among the policy interventions with the strongest estimated impact on child mortality in the country. We investigated how reduced coverage of the BFP and ESF-compared to an alternative scenario where the level of social protection under these programmes is maintained-may affect the under-five mortality rate (U5MR) and socioeconomic inequalities in child health in the country until 2030, the end date of the Sustainable Development Goals.
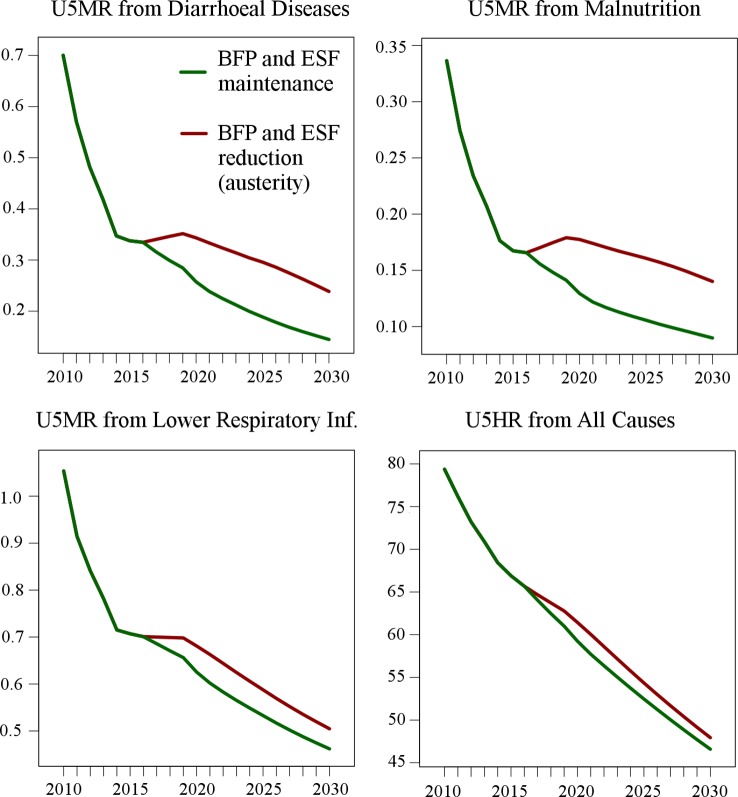
We developed and validated a microsimulation model, creating a synthetic cohort of all 5,507 Brazilian municipalities for the period 2017-2030. This model was based on the longitudinal dataset and effect estimates from a previously published study that evaluated the effects of poverty, the BFP, and the ESF on child health. We forecast the economic crisis and the effect of reductions in BFP and ESF coverage due to current fiscal austerity on the U5MR, and compared this scenario with a scenario where these programmes maintain the levels of social protection by increasing or decreasing with the size of Brazil's vulnerable populations (policy response scenarios). We used fixed effects multivariate regression models including BFP and ESF coverage and accounting for secular trends, demographic and socioeconomic changes, and programme duration effects. With the maintenance of the levels of social protection provided by the BFP and ESF, in the most likely economic crisis scenario the U5MR is expected to be 8.57% (95% CI: 6.88%-10.24%) lower in 2030 than under fiscal austerity-a cumulative 19,732 (95% CI: 10,207-29,285) averted under-five deaths between 2017 and 2030. U5MRs from diarrhoea, malnutrition, and lower respiratory tract infections are projected to be 39.3% (95% CI: 36.9%-41.8%), 35.8% (95% CI: 31.5%-39.9%), and 8.5% (95% CI: 4.1%-12.0%) lower, respectively, in 2030 under the maintenance of BFP and ESF coverage, with 123,549 fewer under-five hospitalisations from all causes over the study period. Reduced coverage of the BFP and ESF will also disproportionately affect U5MR in the most vulnerable areas, with the U5MR in the poorest quintile of municipalities expected to be 11.0% (95% CI: 8.0%-13.8%) lower in 2030 under the maintenance of BFP and ESF levels of social protection than under fiscal austerity, compared to no difference in the richest quintile. Declines in health inequalities over the last decade will also stop under a fiscal austerity scenario: the U5MR concentration index is expected to remain stable over the period 2017-2030, compared to a 13.3% (95% CI: 5.6%-21.8%) reduction under the maintenance of BFP and ESF levels of protection. Limitations of our analysis are the ecological nature of the study, uncertainty around future macroeconomic scenarios, and potential changes in other factors affecting child health. A wide range of sensitivity analyses were conducted to minimise these limitations.
The implementation of fiscal austerity measures in Brazil can be responsible for substantively higher childhood morbidity and mortality than expected under maintenance of social protection-threatening attainment of Sustainable Development Goals for child health and reducing inequality.
自 2015 年以来,巴西经历了一场严重的经济危机,导致贫困加剧,并实施了长期财政紧缩措施,这将在未来 20 年内大幅削减社会福利计划占国内生产总值的比例。Bolsa Família 计划(BFP)——世界上最大的有条件现金转移支付计划之一——以及全国初级卫生保健战略(Estratégia Saúde da Família [ESF])都受到财政紧缩的影响,尽管它们是对该国儿童死亡率产生最强估计影响的政策干预措施之一。我们研究了在维持这些计划的社会保护水平的替代方案下,BFP 和 ESF 的覆盖范围缩小将如何影响该国 2030 年(可持续发展目标的截止日期)之前五岁以下儿童死亡率(U5MR)和儿童健康的社会经济不平等。
我们开发并验证了一个微观模拟模型,为 2017-2030 年期间的所有 5507 个巴西城市创建了一个综合队列。该模型基于纵向数据集和先前发表的研究的效果估计,该研究评估了贫困、BFP 和 ESF 对儿童健康的影响。我们预测了经济危机以及由于当前财政紧缩而导致 BFP 和 ESF 覆盖范围减少对 U5MR 的影响,并将这种情况与这些计划通过增加或减少巴西弱势群体的规模来维持社会保护水平的情况进行了比较(政策应对情景)。我们使用固定效应多元回归模型,包括 BFP 和 ESF 覆盖范围,并考虑到长期趋势、人口和社会经济变化以及计划持续时间的影响。在维持 BFP 和 ESF 提供的社会保护水平的情况下,在最有可能出现的经济危机情景下,预计 2030 年 U5MR 比财政紧缩时低 8.57%(95%CI:6.88%-10.24%)——在 2017 年至 2030 年期间,预计将避免 19732 名(95%CI:10207-29285)五岁以下儿童死亡。预计 2030 年腹泻、营养不良和下呼吸道感染的 U5MR 分别降低 39.3%(95%CI:36.9%-41.8%)、35.8%(95%CI:31.5%-39.9%)和 8.5%(95%CI:4.1%-12.0%),在维持 BFP 和 ESF 覆盖范围的情况下,同期所有病因导致的五岁以下儿童住院治疗将减少 123549 例。BFP 和 ESF 覆盖范围的缩小也将不成比例地影响最脆弱地区的 U5MR,预计最贫困的五分之一城市的 U5MR 在 2030 年将比财政紧缩时低 11.0%(95%CI:8.0%-13.8%),而最富裕的五分之一则没有差异。过去十年中健康不平等的下降也将在财政紧缩的情况下停止:预计 2017-2030 年期间,U5MR 集中指数将保持稳定,而在维持 BFP 和 ESF 保护水平的情况下,该指数将下降 13.3%(95%CI:5.6%-21.8%)。
巴西实施财政紧缩措施可能会导致儿童发病率和死亡率高于预期,这将比维持社会保护更为严重——威胁到实现儿童健康可持续发展目标,并减少不平等。