Department of Surgery, Academic Medical Center, Amsterdam, The Netherlands.
Pancreatic Surgery Unit, Pancreas Translational and Research Institute, Scientific Institute, San Raffaele Hospital, University Vita e Salute, Milan, Italy.
Ann Surg Oncol. 2018 Aug;25(8):2467-2474. doi: 10.1245/s10434-018-6518-2. Epub 2018 May 22.
Despite evidence of different malignant potentials, postoperative follow-up assessment is similar for G1 and G2 pancreatic neuroendocrine tumors (panNETs) and adjuvant treatment currently is not indicated. This study investigated the role of Ki67 with regard to recurrence and survival after curative resection of panNET.
Patients with resected non-functioning panNET diagnosed between 1992 and 2016 from three institutions were retrospectively analyzed. Patients who had G1 or G2 tumor without distant metastases or hereditary syndromes were included in the study. The patients were re-categorized into Ki67 0-5 and Ki67 6-20%. Cox regression analysis with log-rank testing for recurrence and survival was performed.
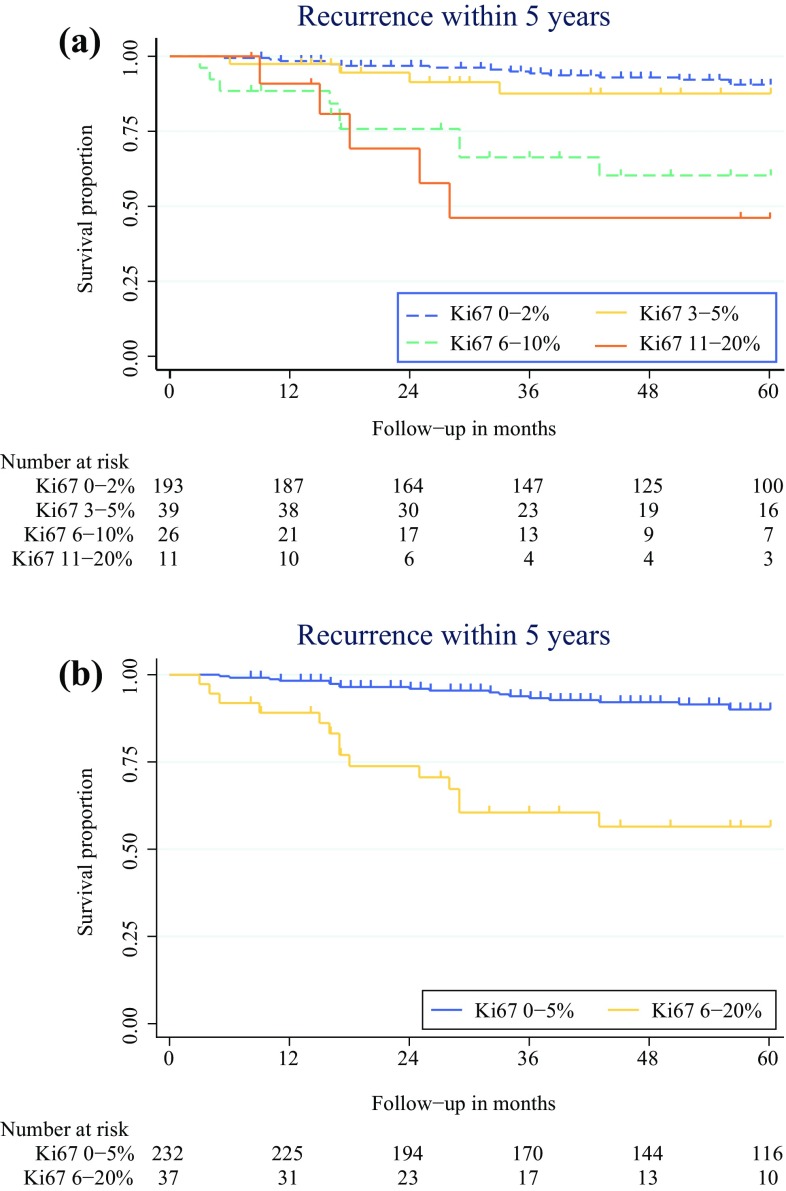
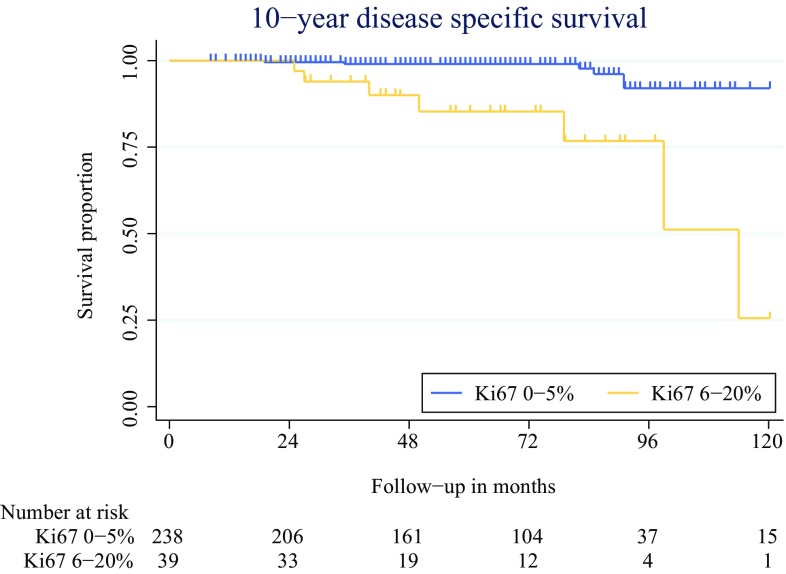
The study enrolled 241 patients (86%) with Ki67 0-5% and 39 patients (14%) with Ki67 6-20%. Recurrence was seen in 34 patients (14%) with Ki67 0-5% after a median period of 34 months and in 16 patients (41%) with Ki67 6-20% after a median period of 16 months (p < 0.001). The 5-year recurrence-free and 10-year disease-specific survival periods were respectively 90 and 91% for Ki67 0-5% and respectively 55 and 26% for Ki67 6-20% (p < 0.001). The overall survival period after recurrence was 44.9 months, which was comparable between the two groups (p = 0.283). In addition to a Ki67 rate higher than 5%, tumor larger than 4 cm and lymph node metastases were independently associated with recurrence.
Patients at high risk for recurrence after curative resection of G1 or G2 panNET can be identified by a Ki67 rate higher than 5%. These patients should be more closely monitored postoperatively to detect recurrence early and might benefit from adjuvant treatment. A clear postoperative follow-up regimen is proposed.
尽管有不同恶性潜能的证据,但 G1 和 G2 胰腺神经内分泌肿瘤(panNET)的术后随访评估相似,目前不建议辅助治疗。本研究调查了 Ki67 在 panNET 根治性切除术后复发和生存方面的作用。
回顾性分析了 3 家机构 1992 年至 2016 年间诊断的切除的无功能 panNET 患者。纳入研究的患者为无远处转移或遗传性综合征的 G1 或 G2 肿瘤患者。患者被重新分类为 Ki67 0-5%和 Ki67 6-20%。使用对数秩检验进行 Cox 回归分析复发和生存。
该研究纳入了 241 例 Ki67 0-5%患者(86%)和 39 例 Ki67 6-20%患者(14%)。Ki67 0-5%患者的中位随访时间为 34 个月,有 34 例(14%)患者复发;Ki67 6-20%患者的中位随访时间为 16 个月,有 16 例(41%)患者复发(p<0.001)。Ki67 0-5%患者的 5 年无复发生存率和 10 年疾病特异性生存率分别为 90%和 91%,Ki67 6-20%患者分别为 55%和 26%(p<0.001)。复发后的总生存时间为 44.9 个月,两组之间无差异(p=0.283)。除 Ki67 率高于 5%外,肿瘤大于 4cm 和淋巴结转移也是复发的独立相关因素。
Ki67 率高于 5%的 G1 或 G2 panNET 根治性切除术后高复发风险的患者可以识别出来。这些患者术后应更密切监测以早期发现复发,并可能受益于辅助治疗。提出了明确的术后随访方案。