Intensive Care Unit and Department of Anesthesiology, Instituto do Cancer, Hospital das Clinicas da Faculdade de Medicina da Universidade de Sao Paulo, Sao Paulo, Brazil.
Department of Anesthesia and Intensive Care, IRCCS San Raffaele Scientific Institute, Milan, Italy.
Crit Care. 2018 May 23;22(1):133. doi: 10.1186/s13054-018-2055-4.
Perioperative goal-directed hemodynamic therapy (GDHT) has been advocated in high-risk patients undergoing noncardiac surgery to reduce postoperative morbidity and mortality. We hypothesized that using cardiac index (CI)-guided GDHT in the postoperative period for patients undergoing high-risk surgery for cancer treatment would reduce 30-day mortality and postoperative complications.
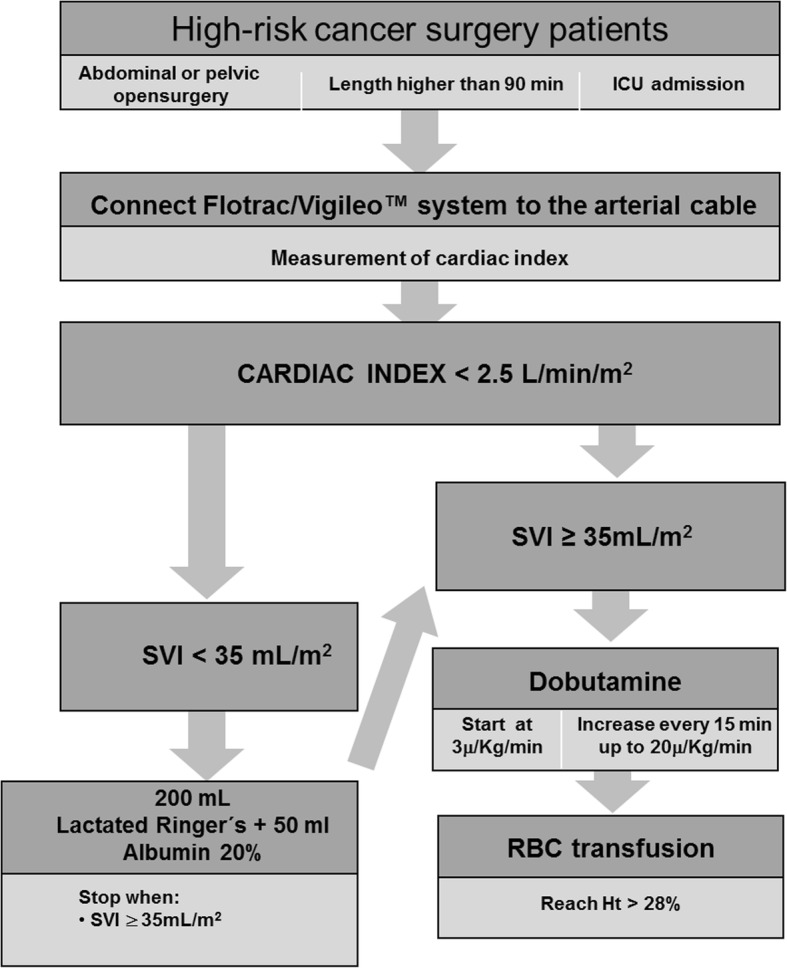
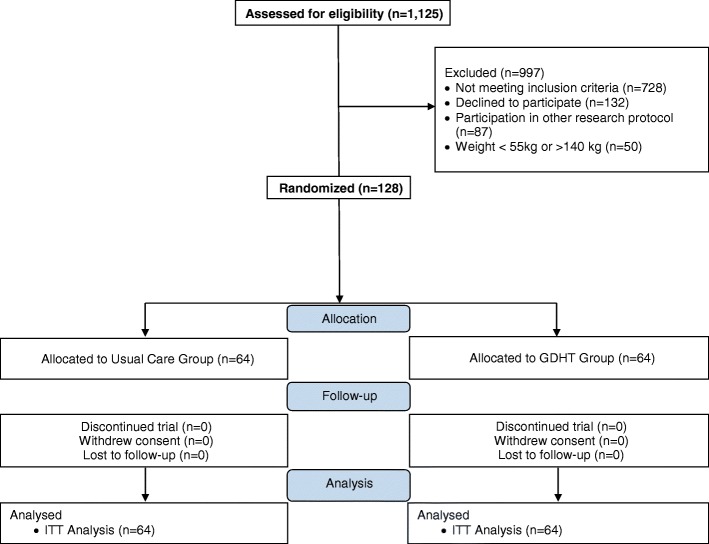
A randomized, parallel-group, superiority trial was performed in a tertiary oncology hospital. All adult patients undergoing high-risk cancer surgery who required intensive care unit admission were randomly allocated to a CI-guided GDHT group or to a usual care group. In the GDHT group, postoperative therapy aimed at CI ≥ 2.5 L/min/m using fluids, inotropes and red blood cells during the first 8 postoperative hours. The primary outcome was a composite endpoint of 30-day all-cause mortality and severe postoperative complications during the hospital stay. A meta-analysis was also conducted including all randomized trials of postoperative GDHT published from 1966 to May 2017.
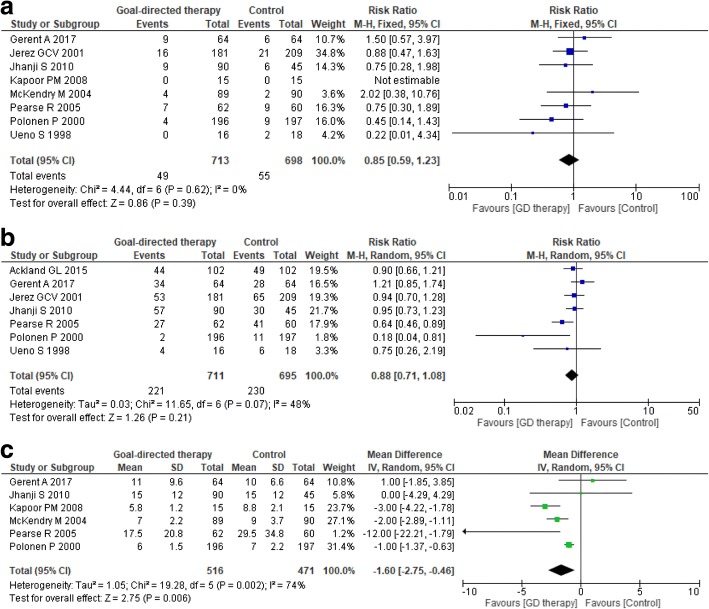
A total of 128 patients (64 in each group) were randomized. The primary outcome occurred in 34 patients of the GDHT group and in 28 patients of the usual care group (53.1% vs 43.8%, absolute difference 9.4 (95% CI, - 7.8 to 25.8); p = 0.3). During the 8-h intervention period more patients in the GDHT group received dobutamine when compared to the usual care group (55% vs 16%, p < 0.001). A meta-analysis of nine randomized trials showed no differences in postoperative mortality (risk ratio 0.85, 95% CI 0.59-1.23; p = 0.4; p for heterogeneity = 0.7; I = 0%) and in the overall complications rate (risk ratio 0.88, 95% CI 0.71-1.08; p = 0.2; p for heterogeneity = 0.07; I = 48%), but a reduced hospital length of stay in the GDHT group (mean difference (MD) - 1.6; 95% CI - 2.75 to - 0.46; p = 0.006; p for heterogeneity = 0.002; I = 74%).
CI-guided hemodynamic therapy in the first 8 postoperative hours does not reduce 30-day mortality and severe complications during hospital stay when compared to usual care in cancer patients undergoing high-risk surgery.
www.clinicaltrials.gov , NCT01946269 . Registered on 16 September 2013.
围手术期目标导向的血流动力学治疗(GDHT)已被提倡用于接受非心脏手术的高危患者,以降低术后发病率和死亡率。我们假设,在接受高危癌症手术治疗的患者中,在术后使用心脏指数(CI)指导的 GDHT 可以降低 30 天死亡率和术后并发症。
在一家三级肿瘤医院进行了一项随机、平行组、优效性试验。所有需要入住重症监护病房的接受高危癌症手术的成年患者均被随机分配到 CI 指导的 GDHT 组或常规治疗组。在 GDHT 组中,在术后的头 8 小时内,通过使用液体、正性肌力药和红细胞,将术后治疗目标设定为 CI≥2.5 L/min/m。主要结局是 30 天内全因死亡率和住院期间严重术后并发症的复合终点。还进行了一项荟萃分析,纳入了 1966 年至 2017 年 5 月发表的所有术后 GDHT 的随机试验。
共有 128 名患者(每组 64 名)被随机分配。GDHT 组有 34 名患者和常规治疗组有 28 名患者发生主要结局(53.1% vs 43.8%,绝对差异 9.4(95%CI,-7.8 至 25.8);p=0.3)。在 8 小时干预期间,GDHT 组接受多巴酚丁胺的患者多于常规治疗组(55% vs 16%,p<0.001)。对 9 项随机试验的荟萃分析显示,术后死亡率无差异(风险比 0.85,95%CI 0.59-1.23;p=0.4;异质性 p=0.7;I=0%)和总体并发症发生率无差异(风险比 0.88,95%CI 0.71-1.08;p=0.2;异质性 p=0.07;I=48%),但 GDHT 组的住院时间缩短(平均差值(MD)-1.6;95%CI -2.75 至 -0.46;p=0.006;异质性 p=0.002;I=74%)。
与高危手术癌症患者的常规治疗相比,在术后头 8 小时内使用 CI 指导的血流动力学治疗并不能降低 30 天死亡率和住院期间的严重并发症。
www.clinicaltrials.gov,NCT01946269。于 2013 年 9 月 16 日注册。