Lorente Juan V, Reguant Francesca, Arnau Anna, Borderas Marcelo, Prieto Juan C, Torrallardona Jordi, Carrasco Laura, Solano Patricia, Pérez Isabel, Farré Carla, Jiménez Ignacio, Ripollés-Melchor Javier, Monge Manuel I, Bosch Joan
Anaesthesia and Critical Care Department, Juan Ramón Jiménez Hospital, Ronda Norte s/n, 21590, Huelva, Spain.
School of Medicine and Health Sciences, International University of Catalonia (UIC), Barcelona, Spain.
Perioper Med (Lond). 2022 Aug 10;11(1):46. doi: 10.1186/s13741-022-00277-w.
Goal-directed haemodynamic therapy (GDHT) has been shown to reduce morbidity and mortality in high-risk surgical patients. However, there is little evidence of its efficacy in patients undergoing hip fracture surgery. This study aims to evaluate the effect of GDHT guided by non-invasive haemodynamic monitoring on perioperative complications in patients undergoing hip fracture surgery.
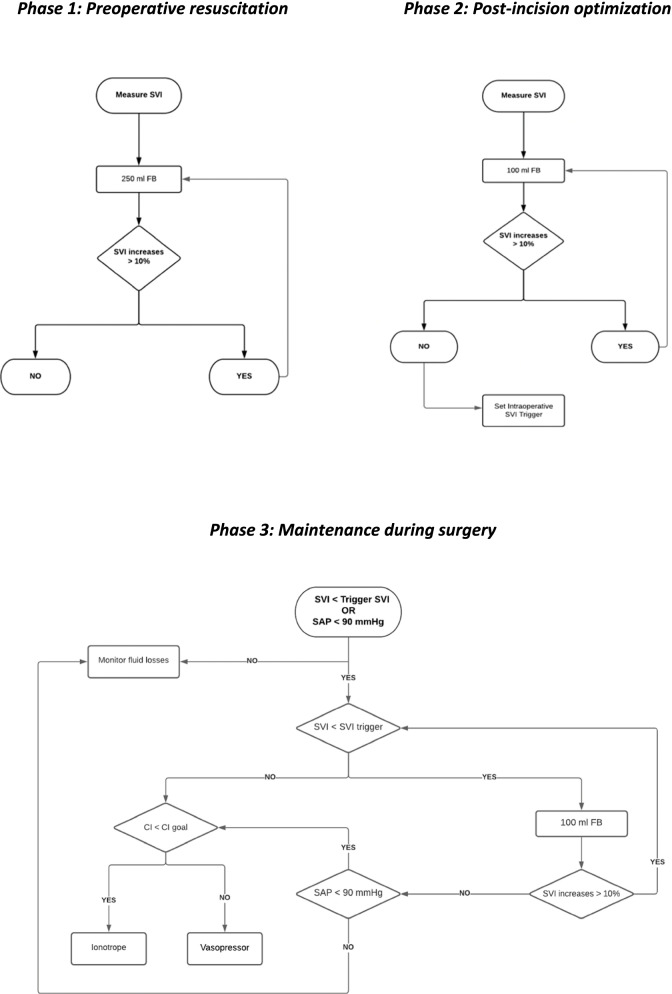
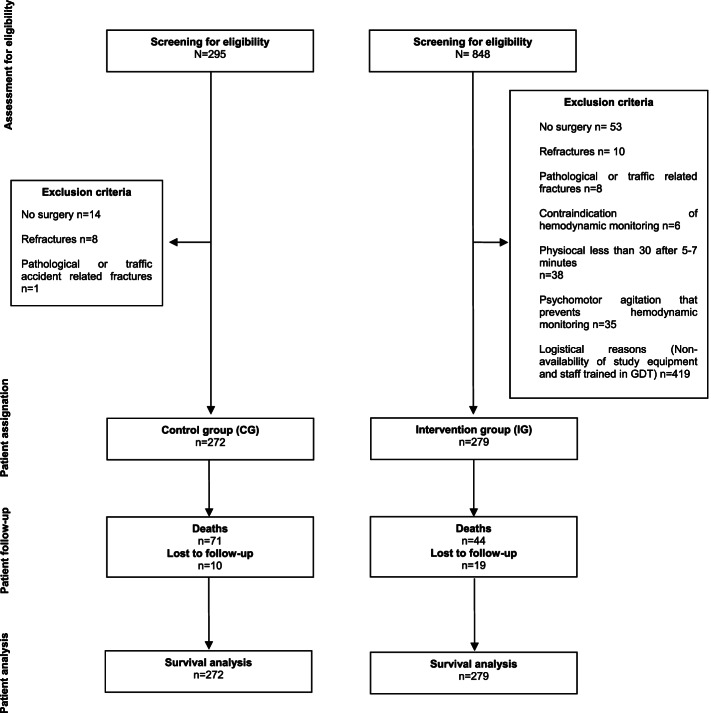
Patients > 64 years undergoing hip fracture surgery within an enhanced recovery pathway (ERP) were enrolled in this single-centre, non-randomized, intervention study with a historical control group and 12-month follow-up. Exclusion criteria were patients with pathological fractures, traffic-related fractures and refractures. Control group (CG) patients received standard care treatment. Intervention group (IG) patients received a GDHT protocol based on achieving an optimal stroke volume, in addition to a systolic blood pressure > 90 mmHg and an individualized cardiac index. No changes were made between groups in the ERP during the study period. Primary outcome was percentage of patients who developed intraoperative haemodynamic instability. Secondary outcomes were intraoperative arrhythmias, postoperative complications (cardiovascular, respiratory, infectious and renal complications), administered fluids, vasopressor requirements, perioperative transfusion, length of hospital stay, readmission and 1-year survival.
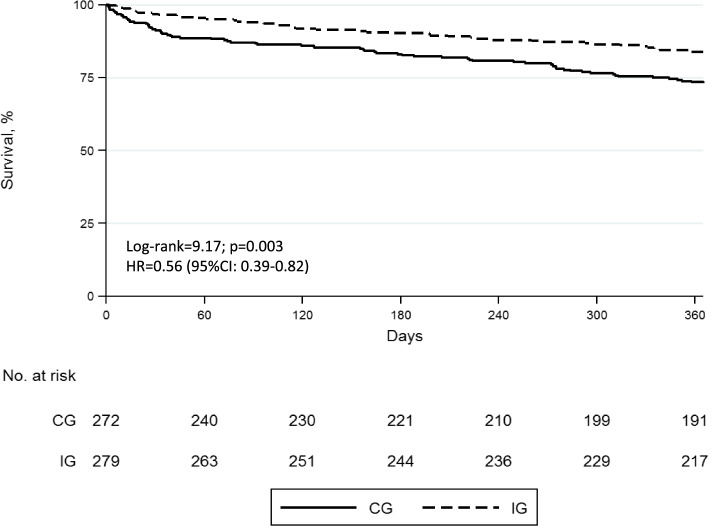
In total, 551 patients (CG=272; IG=279) were included. Intraoperative haemodynamic instability was lower in the IG (37.5% vs 28.0%; p=0.017). GDHT patients had fewer postoperative cardiovascular (18.8% vs 7.2%; p < 0.001), respiratory (15.1% vs 3.6%; p<0.001) and infectious complications (21% vs 3.9%; p<0.001) but not renal (12.1% vs 33.7%; p<0.001). IG patients had less vasopressor requirements (25.5% vs 39.7%; p<0.001) and received less fluids [2.600 ml (IQR 1700 to 2700) vs 850 ml (IQR 750 to 1050); p=0.001] than control group. Fewer patients required transfusion in GDHT group (73.5% vs 44.4%; p<0.001). For IG patients, median length of hospital stay was shorter [11 days (IQR 8 to 16) vs 8 days; (IQR 6 to 11) p < 0.001] and 1-year survival higher [73.4% (95%CI 67.7 to 78.3 vs 83.8% (95%CI 78.8 to 87.7) p<0.003].
The use of GDHT decreases intraoperative complications and postoperative cardiovascular, respiratory and infectious but not postoperative renal complications. This strategy was associated with a shorter hospital stay and increased 1-year survival.
ClinicalTrials.gov NCT02479321 .
目标导向血流动力学治疗(GDHT)已被证明可降低高危手术患者的发病率和死亡率。然而,几乎没有证据表明其在髋部骨折手术患者中有效。本研究旨在评估无创血流动力学监测指导下的GDHT对髋部骨折手术患者围手术期并发症的影响。
本单中心、非随机、干预性研究纳入年龄>64岁且在强化康复路径(ERP)下接受髋部骨折手术的患者,并设立历史对照组,随访12个月。排除标准为病理性骨折患者、交通伤相关骨折患者和再骨折患者。对照组(CG)患者接受标准护理治疗。干预组(IG)患者除收缩压>90 mmHg和个体化心脏指数外,还接受基于达到最佳每搏输出量设定的GDHT方案。研究期间,两组在ERP方面无变化。主要结局是发生术中血流动力学不稳定的患者百分比。次要结局包括术中心律失常、术后并发症(心血管、呼吸、感染和肾脏并发症)、补液量、血管升压药使用需求、围手术期输血、住院时间、再入院率和1年生存率。
共纳入551例患者(CG = 272例;IG = 279例)。干预组术中血流动力学不稳定发生率较低(37.5% 对28.0%;p = 0.017)。接受GDHT治疗的患者术后心血管并发症(18.8% 对7.2%;p < 0.001)、呼吸并发症(15.1% 对3.6%;p < 0.001)和感染并发症(21% 对3.9%;p < 0.001)较少,但肾脏并发症无差异(12.1% 对33.7%;p < 0.001)。与对照组相比,干预组患者血管升压药使用需求较少(25.5% 对39.7%;p < 0.001),补液量也较少[2600 ml(四分位间距1700至2700)对850 ml(四分位间距750至1050);p = 0.001]。GDHT组需要输血的患者较少(73.5% 对44.4%;p < 0.001)。干预组患者的中位住院时间较短[11天(四分位间距8至16)对8天;(四分位间距6至11)p < 0.001],1年生存率较高[73.4%(95%置信区间67.7至78.3)对83.8%(95%置信区间78.8至87.7)p < 0.003]。
使用GDHT可降低术中并发症以及术后心血管、呼吸和感染并发症,但不能降低术后肾脏并发症。该策略与缩短住院时间和提高1年生存率相关。
ClinicalTrials.gov NCT02479321 。