Dushianthan Ahilanandan, Knight Martin, Russell Peter, Grocott Michael Pw
General Intensive Care Unit, University Hospital Southampton NHS Foundation Trust, Southampton, SO16 6YD UK.
Anaesthesia Perioperative and Critical Care Research Group, Southampton NIHR Biomedical Research Centre, University Hospital Southampton/University of Southampton, Southampton, UK.
Perioper Med (Lond). 2020 Oct 15;9:30. doi: 10.1186/s13741-020-00161-5. eCollection 2020.
Perioperative goal-directed haemodynamic therapy (GDHT), defined as the administration of fluids with or without inotropes or vasoactive agents against explicit measured goals to augment blood flow, has been evaluated in many randomised controlled trials (RCTs) over the past four decades. Reported post-operative pulmonary complications commonly include chest infection or pneumonia, atelectasis, acute respiratory distress syndrome or acute lung injury, aspiration pneumonitis, pulmonary embolism, and pulmonary oedema. Despite the substantial clinical literature in this area, it remains unclear whether their incidence is reduced by GDHT. This systematic review aims to determine the effect of GDHT on the respiratory outcomes listed above, in surgical patients.
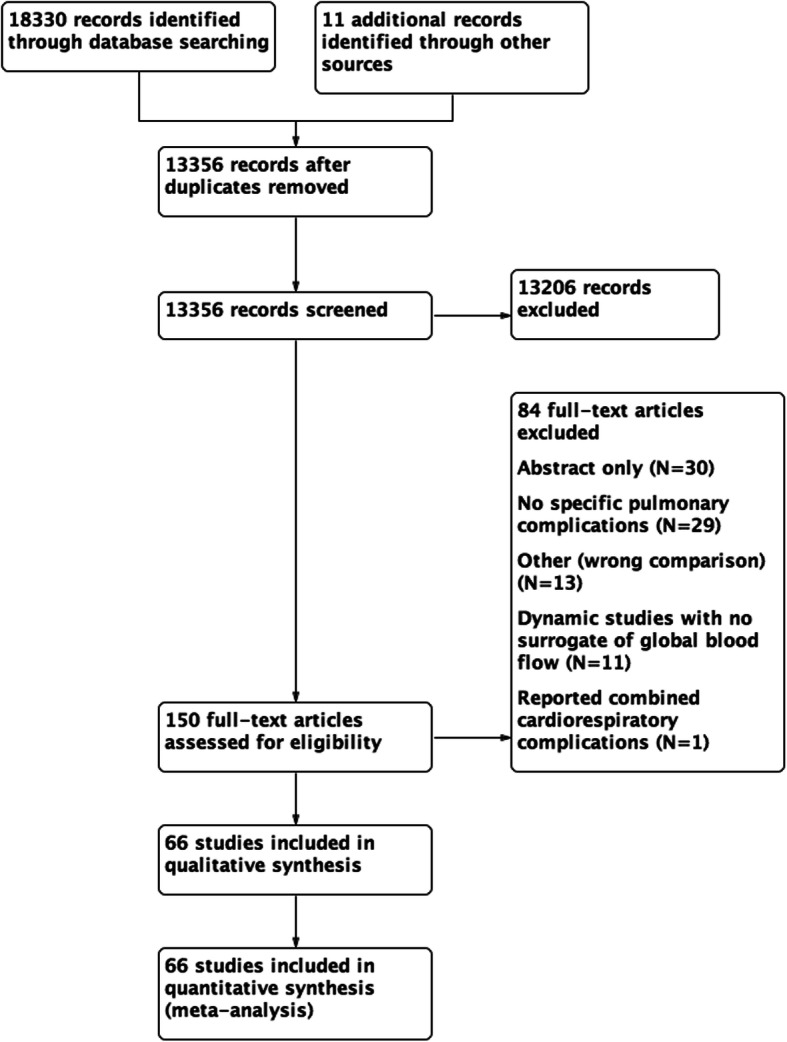
We searched the Cochrane Central Register for Controlled Trials (CENTRAL), MEDLINE, EMBASE, and clinical trial registries up until January 2020. We included all RCTs reporting pulmonary outcomes. The primary outcome was post-operative pulmonary complications and secondary outcomes were specific pulmonary complications and intra-operative fluid input. Data synthesis was performed on Review Manager and heterogeneity was assessed using statistics.
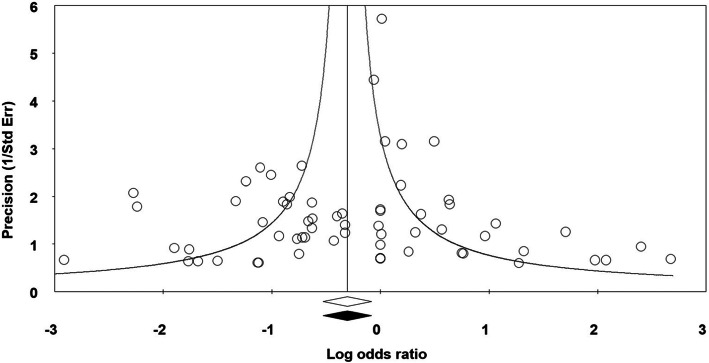
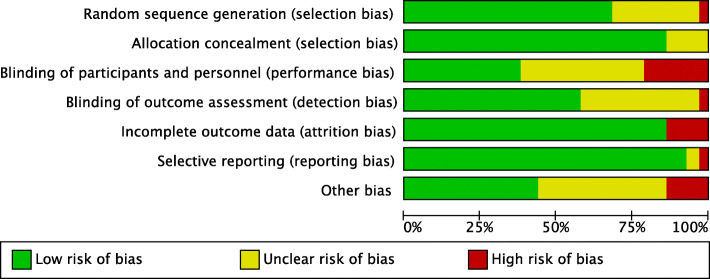
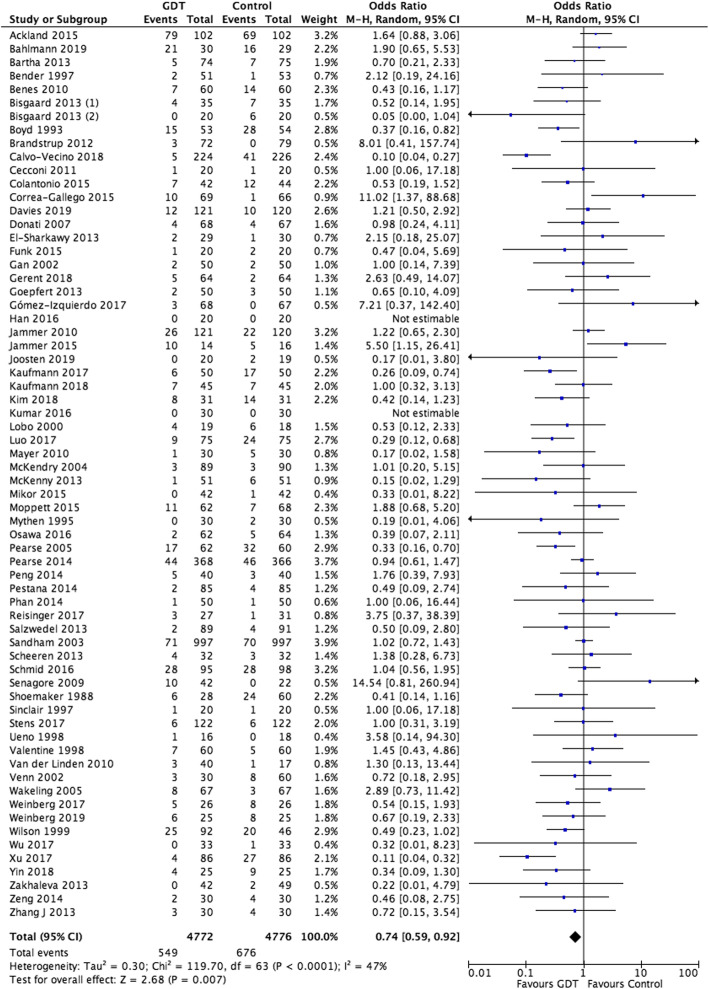
We identified 66 studies with 9548 participants reporting pulmonary complications. GDHT resulted in a significant reduction in total pulmonary complications (OR 0.74, 95% CI 0.59 to 0.92). The incidence of pulmonary infections, reported in 45 studies with 6969 participants, was significantly lower in the GDHT group (OR 0.72, CI 0.60 to 0.86). Pulmonary oedema was recorded in 23 studies with 3205 participants and was less common in the GDHT group (OR 0.47, CI 0.30 to 0.73). There were no differences in the incidences of pulmonary embolism or acute respiratory distress syndrome. Sub-group analyses demonstrated: (i) benefit from GDHT in general/abdominal/mixed and cardiothoracic surgery but not in orthopaedic or vascular surgery; and (ii) benefit from fluids with inotropes and/or vasopressors in combination but not from fluids alone. Overall, the GDHT group received more colloid (+280 ml) and less crystalloid (-375 ml) solutions than the control group. Due to clinical and statistical heterogeneity, we downgraded this evidence to moderate.
This systematic review and meta-analysis suggests that the use of GDHT using fluids with inotropes and/or vasopressors, but not fluids alone, reduces the development of post-operative pulmonary infections and pulmonary oedema in general, abdominal and cardiothoracic surgical patients. This evidence was graded as moderate.PROSPERO registry reference: CRD42020170361.
围手术期目标导向血流动力学治疗(GDHT)定义为根据明确的测量目标给予液体,同时或不使用正性肌力药物或血管活性药物以增加血流量,在过去四十年中已在许多随机对照试验(RCT)中进行了评估。报告的术后肺部并发症通常包括胸部感染或肺炎、肺不张、急性呼吸窘迫综合征或急性肺损伤、吸入性肺炎、肺栓塞和肺水肿。尽管该领域有大量临床文献,但尚不清楚GDHT是否能降低其发生率。本系统评价旨在确定GDHT对手术患者上述呼吸结局的影响。
我们检索了截至2020年1月的Cochrane对照试验中央注册库(CENTRAL)、MEDLINE、EMBASE和临床试验注册库。我们纳入了所有报告肺部结局的RCT。主要结局是术后肺部并发症,次要结局是特定肺部并发症和术中液体输入量。使用Review Manager进行数据合成,并使用统计学方法评估异质性。
我们确定了66项研究,共9548名参与者报告了肺部并发症。GDHT导致总肺部并发症显著减少(OR 0.74,95%CI 0.59至0.92)。在45项研究、6969名参与者中报告的肺部感染发生率,GDHT组显著更低(OR 0.72,CI 0.60至0.86)。在23项研究、3205名参与者中记录了肺水肿,GDHT组中较少见(OR 0.47,CI 0.30至0.73)。肺栓塞或急性呼吸窘迫综合征的发生率没有差异。亚组分析表明:(i)在普通/腹部/混合和心胸外科手术中GDHT有益,但在骨科或血管外科手术中并非如此;(ii)联合使用含正性肌力药物和/或血管升压药物的液体有益,但单独使用液体则不然。总体而言,GDHT组比对照组接受更多胶体溶液(+280毫升)和更少晶体溶液(-375毫升)。由于临床和统计异质性,我们将此证据降级为中等质量。
本系统评价和荟萃分析表明,使用含正性肌力药物和/或血管升压药物的液体进行GDHT(而非仅使用液体)可降低普通、腹部和心胸外科手术患者术后肺部感染和肺水肿的发生率。该证据等级为中等质量。PROSPERO注册编号:CRD42020170361。